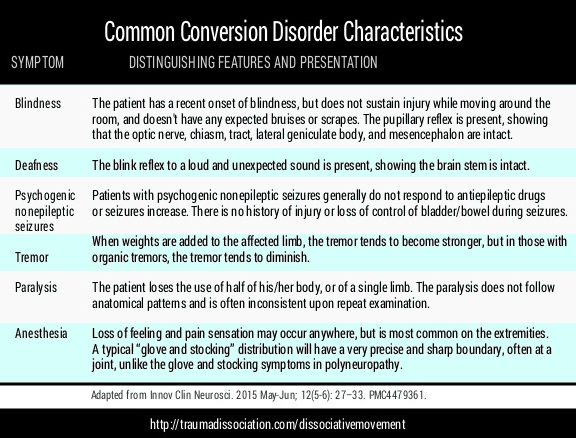
Conversion symptoms are altered motor or sensory functioning, which may include pseudoseizures, either with or without impaired consciousness. In the ICD-10 diagnostic manual, the different types of Conversion Disorder are referred to as Dissociative Disorders of Movement and Sensation. Conversion Disorder is also known as Functional Neurological Symptom Disorder (FND).[1]:1345 Some forms of conversion disorder are referred to as psychogenic disorders, e.g., Psychogenic Blindness. Psychogenic disorders have physical symptoms only, but the symptoms are caused unintentionally and unknowingly as a result of the person's state of mind. The term 'psychogenic' suggests that psychological factors are the sole cause, and ignores the role of biological factors.
Unexplained, but Involuntary symptoms
Conversion Disorder symptoms cannot be fully explained by neurological or other medical conditions, or by substance use, and are not intentionally produced. A psychological stressor is not essential for diagnosis but can is often specified. A separate diagnosis of Factitious Disorder is given if symptoms are feigned/malingered. [1]:627-628, [2] Symptoms may be inconsistent, often changing during examination and/or with a person's level of stress.[2], [6] An accepting rather than judgmental approach towards symptoms is helpful.[6]
How Common is Conversion Disorder?
Although brief periods of conversion symptoms are common, persistent individual conversion symptoms are very rare in the general population, occurring at approximately 2-5 people per 100,000 per year. Conversion disorder is found in approximately 5% of referrals to neurology clinics.[1]:630
Non-epileptic seizures are most common in a person's 30s, and motor symptoms in a person's 40s.
Neurological disorders that cause similar symptoms, e.g. non-epileptic seizures are in people with epilepsy
History of childhood abuse/ neglect
Stressful life events often present
2-3 times more common in females [1]:629-630
Common Forms of Conversion Disorder
Psychogenic nonepileptic seizures (PNES)
These pseudoseizures may resemble epileptic seizures, and may include abnormal generalized limb shaking with impaired/loss of consciousness
episodes of unresponsiveness may occur resembling fainting (syncope) or coma
Sensory symptoms
altered, reduced or absent skin sensations
blindness, or altered/reduced vision
double vision (diplopia)
deafness, or altered/reduced hearing
sensations of a lump in the throat (globus)
Motor (Movement) symptoms
weakness
paralysis
abnormal gait or limb posturing
tremor or abnormal movements
Speech changes
reduced speech volume
inability to speak (aphonia)
altered articulation (dysarthia)
Neuroimaging of Conversion Disorder
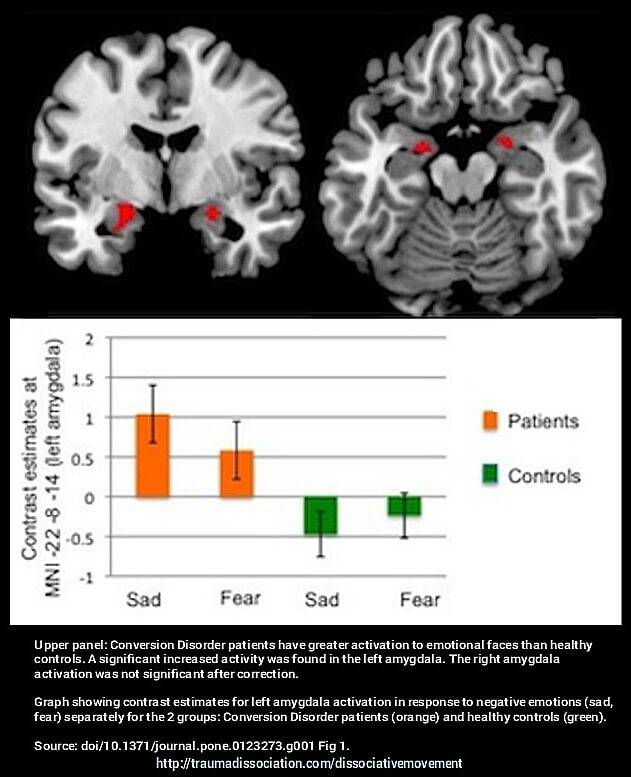
Recent research has shown differences in brain activation in people with Conversion Disorder compared to Healthy Controls.[7] This does not mean that permanent 'brain damage' has occurred, the test results show only that the brain is working in a different way, for example viewing faces with negative emotions causes different brain activation responses, as shown in the picture.
Treating Conversion Disorder can gradually alter this pattern, even 'talking therapy' alone has been shown to be effective in altering and improving brain activation patterns, for example in Posttraumatic Stress Disorder.
Possible Causes or Contributors
Biological Factors Excessive cortisol arousal and impaired communication within the brain can inhibit awareness of bodily sensations. Subtle impairments may be found on neuropsychological tests.
Psychoanalytical Factors Symptoms have a symbolic relationship to an unconscious psychological conflict, e.g., vaginisms protect the patient from expressing unacceptable sexual desires.
Learning Theory Symptoms of illness learned in childhood can begin as a way of coping with an impossible situation. It is often associated with dissociative symptoms, e.g., Depersonalization/Derealization and Dissociative Amnesia either at onset or during symptomatic periods.
Prognosis
Children and adolescents often fare better than adults
Short duration of symptoms and accepting the diagnosis appear to improve outcomes
'Maladaptive' personality traits, co-occurring physical illness and receipt of disability benefits may worsen the outcomes
Onset may begin after either physical trauma (e.g, injury) or psychological trauma
Treating Conversion Disorder: A Case Study
Even when a clear psychological cause is known, some physical treatment may be helpful in combination with 'talking therapy', as described in this case.
The Conversion Disorder hand tremor shown in the video occurred in a 13-year-old girl, who was treated with both a customized wrist brace and psychological therapy using Cognitive Behavioral Therapy.[6] Her severe 'psychogenic tremor' was diagnosed as a Dissociative Motor Disorder and was video taped at different stages during treatment. The videos were useful in showing the girl clear evidence of her improvements.[6] The cause was psychological: severe performance and exam anxiety at school, combined with her parents' difficult relationship. Her hand tremor prevented writing and attending school, increasing her avoidance of school.[6]
"Stop pretending" made things worse
The tremor was inconsistent, reducing when her concentration was on something else and would stop when she grasped something, e.g., clasping her hands together. Finding no neurological or physical cause for the tremor, a physiotherapist told her to "stop pretending" which led to prolonged sadness and anger in the girl, and an increase in the tremor.[6] Secondary gain is sometimes referred to in Conversion Disorder - despite not being part of the diagnostic criteria.[1]:628 This means the person's Conversion Disorder causes an indirect benefit - any secondary gain from not needing to attend school was clearly canceled out by her inability to sleep or eat normally due to the tremor, plus the distress it caused her. She was also hospitalized, and agreed to attend the psychiatric unit. Even in cases where secondary gain is present, this should not be used as a basis for diagnosis.[1]:628
Treatment
She had anxiety-reduction sessions, and learned Progressive Muscle Relaxation. Her customized wrist brace to help her write, and she practiced writing daily. This reduced her school anxiety and avoidance, and she began attending again. She also had private lessons in the subjects she struggled with the most. In her treatment it was key for her to understand what triggered the tremor and prevented it from diminishing. [6]
From the girl's perspective, she found what helped most was:
being more active rather than listening to music alone
physical and social activity
identifying and discussing her feelings with others
eventually mastering the relaxation methods to reduce stress,
and attending physical therapy aimed at symptom reduction [6]
This combination of treatment reduced her tremor by 80% during her time in hospital, and two weeks after discharge it was gone.
Dissociative Motor Disorders
Code F44.4
"The commonest varieties of Dissociative Motor Disorder are loss of ability to move the whole or a part of a limb or limbs. Paralysis may be partial, with movements being weak or slow, or complete. Various forms and variable degrees of incoordination (ataxia) may be evident, particularly in the legs, resulting in bizarre gait or inability to stand unaided (astasia-abasia). There may also be exaggerated trembling or shaking of one or more extremities or the whole body. There may be close resemblance to almost any variety of ataxia, apraxia, akinesia, aphonia, dysarthria, dyskinesia, or paralysis." [3]:126 Dissociative Movement Disorder
This includes psychogenic aphonia and psychogenic dysphonia.
Dissociative Convulsions / Pseudoseizures
Code F44.5
"Dissociative convulsions(pseudoseizures) may mimic epileptic seizures very closely in terms of movements, but tongue-biting, serious bruising due to falling, and incontinence of urine are rare in dissociative convulsion, and loss of consciousness is absent or replaced by a state of stupor or trance." [3]:126
Dissociative anaesthesia and sensory loss
Code F44.6
"Anaesthetic areas of skin often have boundaries which make it clear that they are associated more with the patient's ideas about bodily functions than with medical knowledge. There may also be differential loss between the sensory modalities which cannot be due to a neurological lesion. Sensory loss may be accompanied by complaints of paraesthesia. Loss of vision is rarely total in dissociative disorders, and visual disturbances are more often a loss of acuity, general blurring of vision, or "tunnel vision". In spite of complaints of visual loss, the patient's general mobility and motor performance are often surprisingly well preserved. Dissociative deafness and anosmia are far less common than loss of sensation or vision." [3]:126
This includes psychogenic deafnessPsychogenic Deafness.
Mixed Dissociative [conversion] Disorders
Code F44.7
Mixtures of the following disorders should be diagnosed as mixed dissociative [conversion] disorder
:
If the person has a physical disorder involving the nervous system, or is a previously well-adjusted individual with normal family and social relationships, then a probable or provisional diagnosis may be given instead. A probable or provisional diagnosis should remain if it isn't possible to understand why the symptoms have developed, meaning if no link with a psychological cause or environmental trigger has been found. [3]:122
For a definite diagnosis:
"there should be no evidence of physical disorder; and
sufficient must be known about the psychological and social setting and personal relationships of the patient to allow a convincing formulation to be made of the reasons for the appearance of the disorder." [3]:122
Differential diagnosis
The following conditions must be ruled out as causes: early stages of progressive neurological disorders (e.g., multiple sclerosis, systemic lupus erythematosus). Multiple and ill-defined somatic complaints (physical symptoms without a physical cause) should be classified elsewhere, under somatoform disorders or neurasthenia.
Isolated dissociative symptoms which occur only as part of major mental health diagnoses (e.g., schizophrenia or severe depression) should be ruled out. Feigning symptoms (knowlingly pretending to have symptoms which you do not have) can be difficult for clinicians to distinguish from the dissociative disorders involving movement/sensation; clinicians are advised to use detailed observation, obtain an understanding of person's personality, the circumstances when the symptoms first started, and the consequences of recovery versus continued disability. Patients feigning symptoms can stop symptoms at any time they choose.
DSM-5 Conversion Disorder
Code 300.11
Alternative name: Functional Neurological Symptom Disorder
The DSM-5 classifies this is in the Somatic Symptom and Related Disorders sectional.
Diagnostic Criteria
"A. One or more symptoms of altered voluntary motor or sensory function.
B. Clinical findings provide evidence of incompatibility between the symptom and recognized neurological or medical conditions.
C. The symptom or deficit is not better explained by another medical or mental disorder.
D. The symptom or deficit caused clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation."
Specify if:
Specify symptom type: (F44.4)
With weakness or paralysis
With abnormal movement e.g., tremor, dystonic movement, myoclonus, gait disorder (F44.4)
With swallowing symptoms(F44.4)
With speech symptomse.g., dysphonia, slurred speech (F44.5)
With attacks or seizures(F44.6)
With anesthesia or sensory loss (F44.6)
With special sensory symptom e.g. visual, olfactory, or hearing disturbance (F44.7)
With mixed symptoms" [1]:627-628
Specify if:
Acute episode: Symptoms present for less than 6 months.
Persistent: Symptoms occurring for 6 months or more.
World Health Organization. (1992). The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic criteria for research. Retrieved November 17, 2014, from http://www.who.int/classifications/icd/en/GRNBOOK.pdf
Ali, S., Jabeen, S., Pate, R. J., Shahid, M., Chinala, S., Nathani, M., & Shah, R. (2014). Conversion Disorder—Mind versus Body: A Review. Innovations in clinical neuroscience, 12(5-6), 27. PMID: 26155375. PMCID: PMC4479361.
Van der Kruijs, S. J. M., Bodde, N. M. G., Vaessen, M. J., Lazeron, R. H. C., Vonck, K., Boon, P., … Jansen, J. F. A. (2011). Functional connectivity of dissociation in patients with psychogenic non-epileptic seizures. Journal of Neurology, Neurosurgery & Psychiatry, 83(3), 239–247. doi: 10.1136/jnnp-2011-300776