Posttraumatic Stress Disorder (PTSD) is a very common mental health disorder, affecting 8.7% of people during their lifetime. The core PTSD symptoms are:
re-experiencing the trauma psychologically (flashbacks and nightmares)
avoiding reminders of the trauma
emotional numbing
hyperarousal (irritability, being jumpy, or constantly "on alert" - also known as hypervigilant)
Who gets PTSD?
PTSD is also known as Post-traumatic Stress Syndrome (PTSS) and is not caused by normal, everyday stress.[1] PTSD can occur at any age, it can occur during childhood, adolescence, adulthood and old age.[1]:272-277
Posttraumatic stress disorderaffects around 5% of men and 10% of women at some point during their life. Up to one in three people who experience a traumatic event develop PTSD as a result. — National Health Service, UK [20]
PTSD causes different people to react in very different ways, and it can be very disabling. "The disturbance, regardless of its trigger, causes clinically significant distress or impairment in the individual’s social interactions, capacity to work or other important areas of functioning." [18]
Recovery from PTSD
Recovery rates vary: the DSM-5 states around 50% of adults with PTSD may recover within 3 months but some people have PTSD for over a year. In some cases, PTSD has continued for over 50 years,[1]:277 for example in Vietnam war veterans and Holocaust survivors. Santiago et al. (2013) reviewed many studies of PTSD, finding that 50% recovered within 2 years.
As the graph shows, a third of people exposed to trauma develop PTSD (33%), and recovery is significantly quicker in people exposed to unintentional trauma, for example natural disasters, life-threatening illness or accidents.[8] Factors know to hinder recover, or worsen symptoms after trauma include:
reminders of the original trauma
normal 'life stressors', for example unemployment, illness or bereavement
new traumatic experiences
worsening physical declining health or cognitive function (in older people)
Causes of PTSD: 10 common causes. Only a small percentage of people with PTSD are traumatized by combat. Source of data: Spence et al. (2011). PLoS ONE 6(7): e21864. Being female doubles the risk of a person developing PTSD; the reasons for this are not yet understood.[1]
The type of trauma experienced strongly affects the risk of developing PTSD; many studies show that rape causes the highest rates of PTSD,[1],[3] with over 50% of rape survivors affected.
Combat/military service is a less common cause of PTSD than many people expect, as the graph shows (based on research from Australian adults with PTSD in 2011).[45]
Rates of PTSD vary according to the type and duration of military service, along with many other factors affecting all trauma survivors, including the number of previous types of trauma experienced (both civilian and military), physical injuries sustained, whether there was social support after the trauma.[45]
Dissociative PTSD
Dissociative symptoms, such as subjective sense of numbing or detachment, reduced awareness of an individuals surroundings, derealization, depersonalization, and dissociative amnesia, are cardinal features of posttraumatic stress disorder. [24]
There are also three key groups of symptoms in PTSD that include some dissociative experiences, e.g., intrusion symptoms (such as flashbacks) and emotional numbing. Emotional numbing is often referred to as "psychic numbing" or "emotional anesthesia". [23], [24] Despite the variety of dissociative symptoms typically found in PTSD, PTSD with dissociative features is specified only when PTSD also causes persistent or recurrent depersonalization and/or derealization, for example trauma reminders that trigger depersonalization. The DSM-5 code 309.81 is used whether dissociative features or present or not. [1]
The DSM-5 also includes a with dissociative features specifier for when persistent or recurrent depersonalization or derealization occurs as a response to the traumatic stressor. [1], [21]:1145
Depersonalization
Persistent or recurrent experiences of feeling detached from, and as if one were an outside observer of, one's mental processes or body,
e.g., feeling as though one were in a dream, feeling a sense of unreality of self or body or of time moving slowly. [1]:273
Derealization
Persistent or recurrent experiences of feeling unreality of surroundings,
e.g., the world around the individual is experienced as unreal, dreamlike, distant, or distorted. [1]:273
PTSD with dissociative features is known as the dissociative subtype of PTSD, and differs significantly from Complex PTSD, which involves three additional symptoms. [6], [52] As described above, all PTSD involves some dissociative symptoms, so there is not a "non-dissociative PTSD" subtype, it is simply a less dissociative presentation of PTSD.
The dissociative form of PTSD differs from a Dissociative Disorder since the additional criteria for Dissociative Disorders may not be met; however, PTSD is a very common comorbid diagnosis for people with complex Dissociative Disorders including dissociative identity disorder or other specified dissociative disorder.[20]:298
Differences
The dissociative subtype of PTSD is clinically different from severe PTSD. [1]:207 The criteria were summarized by Friedman (2013) as follows:
All the PTSD criteria are met
High levels of depersonalization or derealization are also present
Dissociative symptoms are not linked to substance use or another medical condition
it is found in both children and adults. [43]:28
A substantial study of data from the World Mental Health Surveys found that people with the Dissociative subtype of PTSD had a higher number of major psychiatric disorders (comorbid DSM-IV "Axis I" disorders), for example depression and anxiety.[14] They were also more likely to have a history of child abuse and neglect than those with "regular" PTSD.[6] Wolf et al. (2012) studied both men and women with PTSD, finding that repeated sexual assault or abuse was more common in people with the dissociative subtype of PTSD, both child sexual abuse and adult sexual trauma. The women in this sample were more likely than the men to have avoidant personality disorder or borderline personality disorder diagnoses in addition to PTSD. [17]
Responses to trauma differ in people with the dissociative subtype of PTSD, most people with PTSD react to a personalized "trauma-script" with high levels of psychological distress and related physiological reactions, and greater reexperiencing symptoms (such as flashbacks), but those with the dissociative subtype showed dissociative symptoms but lacked the other these symptoms. [6], [52] For example, they had less awareness of surroundings/zoned out, felt depersonalized or experienced derealization. Brain activity also differed between the two groups.[6]
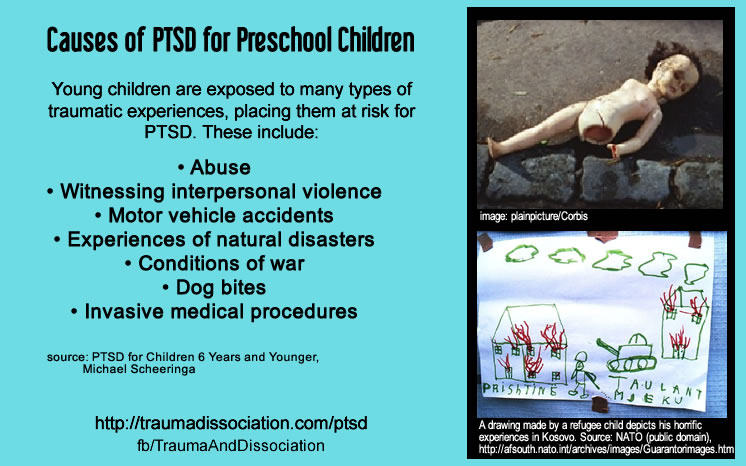
PTSD in Preschool Children
Infants and children aged six years old or younger can be diagnosed with PTSD, but young children's thinking and ability to express themselves in words is limited. This means both their symptoms and diagnostic criteria are slightly different from those in adults or older children.
Most of the research on Preschool PTSD involved three- to six-year-olds, with some studies also including younger children.[13] Babies and toddlers can have PTSD: the minimum age for diagnosis is one year old.[1]:272-274
Posttraumatic Stress Disorder for Children 6 Years and Younger are "developmentally sensitive". Some of the changes from the main PTSD criteria include:
constricted play is an example of "diminished interest in significant activities"
social withdrawal or behavioral changes can indicate "feelings of detachment or estrangement.
extreme temper tantrums are now included with "irritability or outbursts of anger"
intrusive symptoms such as flashbacks and intrusive thoughts do not always manifest overt distress in preschool children
Scheeringa (2014) states that "while distressed reactions are common, parents also commonly reported no affect or what appeared to be excitement" [13]
fewer avoidance symptoms are included because avoidance is internalized, and harder to detect by observation, for example in pre-verbal children
Developmental Trauma Disorder
Developmental Trauma Disorder is a term used to refer to Complex PTSD symptoms in children. [11] Like Complex PTSD it is caused by repeated and/or prolonged periods of trauma, for example child abuse by a familiar person. It was not included in the final DSM-5. [1]
Research has shown preschool children with PTSD have "impaired functioning" in many different areas of life, and the symptoms and impairment are stable in the long-term.[5] Very young children do not simple "bounce back" from PTSD. A study of 70 three- to six-year-olds affected directly by Hurricane Katrina found that children who stayed in New Orleans had significantly higher rates of PTSD than children who were evacuees (62.5%, compared to 43.5%).[12] None of the children who did not develop PTSD developed other mental disorders as a result of the trauma. The children were much more likely to have developed PTSD than their parents/caregivers; the "caregivers' rate of PTSD was 35.6%, of which 47.6% was new post-Katrina". This means that the hurricane's impact nearly doubled the rate of PTSD in the adults, compared to before the trauma.
Effects of PTSD on children
Most children who develop PTSD also develop additional mental disorders (comorbid disorders) as a result of the trauma. In the case of Hurricane Katrina, the most common additional disorders were Oppositional Defiant Disorder and Separation Anxiety Disorder
A study of children 2–6 years old, and 7–10 years old, all traumatized by car crashes/motor vehicle accidents, found many differences between parents' and their children's reports of the trauma and its impact. This shows that relying solely on information from a parent of a traumatized child rather than the child leads to missing key information when assessing PTSD.[7] Given the subjective nature of the experience this is not surprising.
Effective treatments for infants and very young children with PTSD include Cognitive Behavioral Therapy (CBT), long-term, relationally-based therapy (e.g., in cases of interpersonal violence such as child abuse), Play Therapy, Eye Movement Desensitization and Reprocessing (EMDR), and others. Trauma treatment methods need to be developmentally-appropriate to the child's age.
See also: Dissociative form of PTSD
See also: Trauma and abuse
Delayed PTSD
PTSD with delayed expression occurs when the criteria for PTSD are not met for at least 6 months after the trauma; in some cases the onset of PTSD can be years after the trauma. This has been well documented and researched.[18]
A recent systematic review of 19 group studies indicated that delayed accounted for 38.2 and 15.3%, respectively of military and civilian cases of PTSD.[124] PTSD in the absence of any prior symptoms was extremely rare; this analysis found that delayed usually involved subsyndromal PTSD symptoms that later escalated to the full syndrome (possibly because of breakdown of very effective avoidance that previously worked to suppress reexperiencing symptoms and emotions for some period of time).[124] Delayed onset PTSD is very uncommon after natural disasters, but it is not clear whether it is more likely to occur following military rather than non-military trauma.[25]
Complex PTSD
Complex PTSD or C-PTSD is now a diagnosis in the World Health Organization's ICD-11 manual (code 6B41) but is still not in the American DSM-5. Complex PTSD (C-PTSD) is diagnosed all the symptoms of PTSD are fully met plus three additional symptoms:
In addition, Complex PTSD is characterised by severe and persistent
1) problems in affect regulation, e.g., dissociative symptoms when under stress, and the inability to experience positive emotions;
2) beliefs about oneself as diminished, defeated or worthless, accompanied by feelings of shame, guilt or failure related to the traumatic event, e.g., feeling guilty about not having escaped from the situation, or not being able to prevent others from suffering; and
3) difficulties in sustaining relationships and in feeling close to others, e.g., persisent avoidance or detachment in interpersonal relationships or in socializing, or occasional intense relationships they struggle to sustain
These symptoms cause significant impairment in personal, family, social, educational, occupational or other important areas of functioning.[3]
Complex PTSD is most commonly found after prolonged or repetitive events from which escape is difficult or impossible - though this is not a requirement.
Previously Complex PTSD was described inconsistently in psychiatric manuals:
In the DSM-IV PTSD section under the heading PTSD and its Associated Features (APA, 2000),
as Enduring Personality Change after Catastrophic Experience (EPCACE) in the WHO's ICD-10, F62.0, which was a personality disorder that could only be diagnosed after two years of symptoms. [26]
Disorders of Extreme Stress Not Otherwise Specified (DESNOS) was a proposed name for the DSM-IV that was not adopted, but the description was included under the heading PTSD and its Associated Features, which did not include diagnostic criteria
There is a significant relationship between Complex PTSD symptoms and a history of sexual abuse, which is supported by a number of different studies.[27]
Developmental Trauma Disorder (DTD) has been proposed as the child equivalent to Complex PTSD. [11]
This section refers to research from PTSD resulting from a single trauma caused by physical or sexual assault/rape, rather than multiple traumas, although severe and persistent PTSD can be caused by either.
Chronic PTSD refers to PTSD which lasts 3 months or longer, PTSD lasting under 3 months is known as Acute PTSD; this classification was used in the DSM-IV diagnostic manual, but was removed by the DSM-5 changes.[18]:12, [1]:272 Chronic PTSD can vary in severity from mild to severe, but for many people is severe.Acute PTSD can also be severe.
Negative views linked to persistent, chronic PTSD include:
Nowhere is safe
I cannot rely on other people
I can’t trust my own judgments
I am going mad
It was my fault [2]
For example, persistently holding oneself responsible for causing the trauma or not avoiding it, or negative self-judgments about one's instinctive reactions during or after the trauma are linked to a longer duration of PTSD symptoms. These common negative beliefs are a symptoms of the trauma itself,[1]:272 and not an objective truth, sometimes these beliefs can be encouraged by people who wish to maintain their view of a "just world" rather than accept that a similar trauma could happen to them. People who are able to find some positive, for example, recognizing their own ability to have survived both the trauma and the horror of PTSD for so long, and identify positive qualities they did not have or were not aware of before, have a shorter duration to their PTSD. This has been referred to as Post-traumatic Growth (PTG). Besides the factors negative beliefs above, avoiding trauma reminders and seeking safety in order to control PTSD have been associated with more persistent PTSD.[2],[28],[29]
Severe PTSD
The diagnosis of PTSD does not include any description of what counts as mild, moderate or severe,[1]:272 but PTSD assessment tools are available to determine this. Factors during the time of trauma that lead to more severe PTSD:
sense of hopelessness
emotional detachment
confusion [2]
A person's "perceived life threat" and "injury threat" during the trauma were found to be significantly correlated with PTSD severity at 4, 6 and 9 months after the trauma.[2] The person's perceived lack of control during the trauma was related to initial PTSD severity. Dunmore et al. (2001) found that the severity of a physical or sexual assault affected only the initial severity of PTSD, and the number of assailants affected only the longer-term severity (as measured at 9 months); other assault characteristics like time of day, duration of assault and relationship with the assailant were not found to be linked with the severity or persistence of PTSD (although most participants in the research were assaulted by a stranger at night, in a single traumatic event only). [2]
Complex PTSD for PTSD from multiple in erpersonal traumas, including child abuse
PTSD can be caused by "exposure to actual or threatened death or serious injury" either by experiencing it yourself, or by witnessing it.[1] This includes medical illness or events, for example being diagnosed with a serious or potentially terminal illness like cancer or HIV, or witnessing the effect someone else's medical treatment and/or death.[21]:143
PTSD, physical illness and cancer
Posttraumatic stress disorder has been studied in patients with heart problems, hemorrhage and stroke, childbirth, miscarriage, abortion and gynecological procedures, intensive care treatment, HIV infection, cancer and other conditions; with Favaro et al. (2011) finding that 12% of heart transplant recipients suffered PTSD as a result of the transplant. One study, which excluded cancer, found the highest rates were found in patients treated in Intensive Care Units (ICUs), and those with HIV infection. Wade et al. (2013) reviewed a number of studies of patients in critical care, and found risks of PTSD were higher with patients who were sedated for longer, were on mechanical ventilators for longer, were given benzodiazepines, experienced greater levels of fear and stress in the ICU and had frightening memories of admission. Tedstone and Tarrier (2003) found the severity of the physical illness did not predict the risk of PTSD. Posluszny et al. (2011) found that even the perceived threat of cancer caused PTSD; 15% of women with a non-life-threatening gynecologic disease met the diagnostic criteria for PTSD after gynecologic surgery which revealed they did not have cancer.[9]
Survivor Guilt and PTSD
Jim's Story of Survivor Guilt Jim Polehinke was the only survivor of the 2066 Comair crash. He lives with the guilt - and blame. [47]
Witnessing, in person, the events(s) as it occurred to others.
Learning that the traumatic events(s) occurred to a close family member or close friend. In cases of actual or threatened by death of a family member or friend, the events(s) must have been violent or accidental.
Experiencing repeated or extreme exposure to adversive details of the traumatic event(s) (e.g., first responders collecting human remains; police officers repeatedly exposed to details of child abuse). This does not apply to exposure through electronic media, television, movies, or pictures unless this exposure is work related."
B. Presence of one (or more) of the following intrusion symptoms associated with the traumatic event(s) occurred:
Recurrent, involuntary, and intrusive distressing memories of the traumatic event(s). In children older than 6, there may be frightening dreams without recognizable content.
Recurrent distressing dreams in which the content and/or effect of the dream are related to the traumatic event(s).
Dissociative reactions (e.g., flashbacks) in which the individual feels or acts as if the trauma event(s) were recurring. (Such reactions may occur on a continuum, with the most extreme expression being a complete loss of awareness of present surroundings). In children, trauma-specific reenactment may occur in play.
Intense or prolonged psychological distress at exposure to internal or external cues that symbolize or resemble an aspect of the traumatic event(s).
Marked physiological reactions to internal or external cues that symbolize or resemble an aspect of the traumatic event(s)."
C.Persistent avoidance of stimuli associated with the traumatic event(s), beginning after the traumatic event(s) occurred, as evidenced by one or both of the following.
Avoidance of or efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
Avoidance of or efforts to avoid external reminders (people, places, conversations, activities, objects, situations) that arouse distressing memories, thoughts, or feelings about or closely associated with the traumatic event(s).
D.Negative alterations in cognitions and mood associated with the traumatic events(s), beginning or worsening after the traumatic event(s), as evidenced by two (or more) of the following:
Inability to remember an important aspect of the traumatic events(s) (typically due to dissociative amnesia and not to other factors such as head injury, alcohol, or drugs).
Persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (e.g., "I am bad," "no one can be trusted," "the world is completely dangerous," "my whole nervousness system is permanently ruined.").
Persistent, distorted cognitions about the cause or consequences of the traumatic event(s) that lead the individual to blame himself/herself or others.
Persistent negative emotional state (e.g., fear, horror, anger, guilt, or shame).
Markedly diminished interest or participation in significant activities.
Feelings of detachment or estrangement from others.
Persistent inability to experience positive emotions (e.g., inability to experience happiness, satisfaction, or loving feelings).
E.Marked alterations in arousal and reactivity associated with the traumatic event(s), beginning or worsening after the traumatic event(s) occurred, as evidenced by two (or more) of the following.
Irritable behavior and angry outbursts (with little or no provocation) typically expressed as verbal or physical aggression toward people or objects.
Reckless or self-destructive behavior
Hypervigilance
Exaggerated startle response
Problems with concentration
Sleep disturbances
F. Criteria B, C, D and E last more than 1 month.
G. The disturbance causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
H. The disturbance is not attributable to the effects of a substance (e.g., medication, alcohol) or another medical condition.
This must be specified if the full criteria are not met until at least 6 months after the traumatic event; the criteria may be partially met during this time. [1]:272-274
ICD-11 diagnostic criteria
Post traumatic stress disorder
Code 6B40
"Post traumatic stress disorder (PTSD) may develop following exposure to an extremely threatening or horrific event or series of events. It is characterised by all of the following: 1) re-experiencing the traumatic event or events in the present in the form of vivid intrusive memories, flashbacks, or nightmares. Re-experiencing may occur via one or multiple sensory modalities and is typically accompanied by strong or overwhelming emotions, particularly fear or horror, and strong physical sensations; 2) avoidance of thoughts and memories of the event or events, or avoidance of activities, situations, or people reminiscent of the event(s); and 3) persistent perceptions of heightened current threat, for example as indicated by hypervigilance or an enhanced startle reaction to stimuli such as unexpected noises. The symptoms persist for at least several weeks and cause significant impairment in personal, family, social, educational, occupational or other important areas of functioning." [51]
Also known as:
Traumatic Neurosis
Exclusions:
Acute stress reaction (code QE84)
Complex post traumatic stress[51]
ICD-11 Diagnostic criteria
Required Features:
• "Exposure to an event or situation (either short- or long-lasting) of an extremely threatening or horrific nature. Such events include, but are not limited to, directly experiencing natural or human-made disasters,combat, serious accidents, torture, sexual violence, terrorism, assault or acute life-threatening illness (e.g., a heart attack); witnessing the threatened or actual injury or death of others in a sudden, unexpected, or violent manner; and learning about the sudden, unexpected or violent death of a loved one.
• Following the traumatic event or situation, the development of a characteristic syndrome lasting for at least several weeks, consisting of all three core elements:
1. Re-experiencing the traumatic event in the present, in which the event(s) is not just remembered but is experienced as occurring again in the here and now. This typically occurs in the form of vivid intrusive memories or images; flashbacks, which can vary from mild (there is a transient sense of the event occurring again in the present) to severe (there is a complete loss of awareness of present surroundings), or repetitive dreams or nightmares that are thematically related to the traumatic event(s). Re-experiencing is typically accompanied by strong or overwhelming emotions, such as fear or horror, and strong physical sensations. Re-experiencing in the present can also involve feelings of being overwhelmed or immersed in the same intense emotions that were experienced during the traumatic event, without a prominent cognitive aspect, and may occur in response to reminders of the event. Reflecting on or ruminating about the event(s) and remembering the feelings that one experienced at that time are not sufficient to meet the re-experiencing requirement.
2. Deliberate avoidance of reminders likely to produce re-experiencing of the traumatic event(s). This may take the form either of active internal avoidance of thoughts and memories related to the event(s), or external avoidance of people, conversations, activities, or situations reminiscent of the event(s). In extreme cases the person may change their environment (e.g., move house or change jobs) to avoid reminders.
3. Persistent perceptions of heightened current threat, for example as indicated by hypervigilance or an enhanced startle reaction to stimuli such as unexpected noises.
Hypervigilant persons constantly guard themselves against danger and feel themselves or others close to them to be under immediate threat either in specific situations or more generally. They may adopt new behaviours designed to ensure safety (not sitting with ones’ back to the door, repeated checking in vehicles’ rear-view mirrors).
• The disturbance results in significant impairment in personal, family, social, educational, occupational or other important areas of functioning. If functioning is maintained, it is only through significant additional effort.
Additional Clinical Features
PTSD may also include these symptoms:
general dysphoria, dissociative symptoms, somatic complaints, suicidal ideation and behaviour, social withdrawal, excessive alcohol or drug use to avoid re-experiencing or manage emotional reactions, anxiety symptoms including panic, and obsessions or compulsions in response to memories or reminders of the trauma,
anger, shame, sadness, humiliation, or guilt, including survivor guilt, are common. [51]
Course Features:
Onset of PTSD can occur at any time during the life span following exposure to a traumatic event.
PTSD symptoms typically start within three months following a traumatic event, but delayed expression of PTSD can occur even years after a traumatic event.
The symptoms and course of PTSD can vary significantly over time and in different people. Symptoms can reoccur after to exposure to reminders of the traumatic event (triggers) or as a result of additional stress or further traumas. Some people with PTSD have constant symptoms for months or years.
Nearly 50% of people with PTSD will fully recover within 3 months [51]
ICD-10 diagnostic criteria
Code
Post-traumatic stress disorder
"Arises as a delayed or protracted response to a stressful event or situation (of either brief or long duration) of an exceptionally threatening or catastrophic nature, which is likely to cause pervasive distress in almost anyone. Predisposing factors, such as personality traits (e.g. compulsive, asthenic) or previous history of neurotic illness, may lower the threshold for the development of the syndrome or aggravate its course, but they are neither necessary nor sufficient to explain its occurrence.
Typical features include episodes of repeated reliving of the trauma in intrusive memories ("flashbacks"), dreams or nightmares, occurring against the persisting background of a sense of "numbness" and emotional blunting, detachment from other people, unresponsiveness to surroundings, anhedonia, and avoidance of activities and situations reminiscent of the trauma.
There is usually a state of autonomic hyperarousal with hypervigilance, an enhanced startle reaction, and insomnia. Anxiety and depression are commonly associated with the above symptoms and signs, and suicidal ideation is not infrequent. The onset follows the trauma with a latency period that may range from a few weeks to months. The course is fluctuating but recovery can be expected in the majority of cases. In a small proportion of cases the condition may follow a chronic course over many years, with eventual transition to an enduring personality change (F62.0)."
Also known as: Traumatic Neurosis [50]
Changes between the DSM-IV & DSM-5
PTSD is not an Anxiety Disorder
Posttraumatic stress disorder, along with Acute Stress Disorder, have moved from the Anxiety Disorders section to the newly created Trauma- and Stressor-Related Disorders, which recognizes that the symptoms are broader than Anxiety alone. [1] Young children now have separate diagnostic criteria, with the diagnosis being called Posttraumatic Stress Disorder for Children 6 Years and Younger. [1]:272 Chronic and Acute specifiers, which related to the duration of symtoms, are removed.
New PTSD Symptoms in the DSM-5
Negative alterations in cognitions and mood associated with the traumatic events(s) is a new category of symptoms, although some of these were previously included as Avoidance symptoms.
Persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (e.g., "I am bad," "the world is completely dangerous")
erroneous self-blame or blaming others for the trauma
negative mood states (e.g., fear, horror, anger, guilt, or shame)
reckless and maladaptive behavior, e.g. example reckless driving
the irritability symptoms has criterion been changed to aggressive behavior, which includes verbal aggression but does not refer to violence[18] [1]:272-274
illusions and hallucinations have been removed from the examples of trauma symptoms listed in one criteria
the DSM-IV delayed onset specifier has been reworded to delayed expression; this is used when symptoms were delayed for at least 6 months after the trauma. Some PTSD symptoms may begin immediately after the trauma. [1]:273-274
PTSD Symptoms removed
The only significant symptom removed is the optional symptom A sense of a foreshortened future, which means the person doesn't expect to have a career, marriage, children, or a normal life span
PTSD Subtype changes
A new form of PTSD was added to the DSM-5, the PTSD dissociative subtype, which has "prominent dissociative symptoms" which can be either Depersonalization (feeling detached from one’s own mind and/or body), or Derealization (experiencing the world as unreal, dreamlike or having distorted perceptions). [1]
Confusingly, the Dissociative form of PTSD is described as a "subtype" but the diagnostic criteria lists "with dissociative symptoms" is a specifier instead of a subtype. [1]
PTSD Illusions and Hallucinations
The DSM-5 clearly states that "illusions and hallucinations" can be PTSD symptoms. A particular type of auditory pseudo-hallucination, hearing your own thoughts spoken out loud in one or more voices, which may be described as hearing voices, is a recognized feature of PTSD. Paranoia (paranoid ideation) is also a possible result of PTSD.[1]:276
This improves upon the "Notes on flashbacks and psychotic hallucinations" section which was in the additional information in the PTSD section of the DSM-IV-TR and stated the importance of distinguishing between flashbacks and psychotic hallucinations:
"Flashbacks in Posttraumatic Stress Disorder must be distinguished from illusions, hallucinations, and other perceptual disturbances that may occur in Schizophrenia, other Psychotic Disorders, Mood Disorder with Psychotic features, a delirium, Substance-Induced Disorders, and Psychotic Disorders Due to a General Medical Condition." [22]:467
Traumatic Bereavement and PTSD
This happens when PTSD is caused by the death of a loved one in sudden or distressing circumstances, e.g. suicide, murder or witnessing the death in traumatic circumstances.
See Traumatic Bereavement
Denial of PTSD
People with posttraumatic stress disorder may experience denial about the condition, in addition to amnesia, avoidance, minimization of the effects of the trauma and/or cognitive impairment. Each of these can affect whether the person will be diagnosed with PTSD, and the severity determined. "Collateral reports" can be used to add information from spouses/partners, friends or family and from prior medical reports. The spouse/partner (S/P) Mississippi scale was developed to aid collateral assessment [30]:264-265
Some clinicians may at times minimize the effects of the trauma, or fail to recognize trauma which is not in the given examples of types of trauma for diagnosis (e.g., threatened death, serious injury, war, rape or sexual violence or witnessing a major trauma). Cash (2006) states that even a clinician who is aware of the trauma and PTSD symptoms may deny the PTSD diagnosis. Writing in 1997, Cash stated that "most mental health professionals do not receive much (if any) training or experience with [trauma] disorders during their graduate training."[1]:290 [31]:4-5 This could be because PTSD was not given a separate category in the DSM until 1980; although "traumatic stress" was included from the first edition.
Comorbid disorders
It is typical for people with PTSD to have other disorders which are caused by the effects of the trauma.[45] Approximately 80% of people also have other mental disorders, and a persistent "negative mood" or inability to feel positive emotions is part of the diagnostic criteria. Unsurprisingly, Depression (Major Depressive Disorder and other forms), Anxiety Disorders and Substance Misuse (alcoholism, addiction to or misuse of drugs, including prescription medication) are the most common disorders.[45] Many people with Borderline Personality Disorder have PTSD, and a history of childhood physical or sexual abuse is fairly common in people with PTSD.[20]:685
Most people with Dissociative Identity Disorder also have PTSD, although rates of Dissociative Identity Disorder and Dissociative Disorders are significantly lower than PTSD. Dissociative Identity Disorder is caused by childhood trauma only.[20]:278
PTSD and Suicide Risk
The suicide risk is increased in people who have experienced trauma, with those who have PTSD being at greater risk of suicide compared to those who did not develop PTSD after the trauma. PTSD is associated with both suicide attempts and suicidal ideation. [20]:278, 803
Traumatic Brain Injury, ASD & PTSD
Major or Mild Neurocognitive Disorder Due to Traumatic Brain Injury, commonly known as TBI, is a neurocognitive disorder (NCD), which results from physical injury to the head. Traumatic brain injury is either "a traumatically induced structural injury" or "physiological disruption of brain function", caused as a result of an external force. [37] TBI causes some people mental/behavioral symptoms (e.g., depression, personality changes like aggression) as well as neurological/cognitive symptoms (e.g., impaired concentration).[1]:264, [1]:266-276 It can be comorbid with PTSD when the trauma involves a physical head injury, e.g., bomb blasts, physical assault, or auto accidents. [1]:323 Many symptoms overlap with PTSD; the combination of TBI and PTSD is particularly common in military veterans. [38]
Some symptoms of Traumatic Brain Injury which are not present in PTSD include loss of consciousness immediately after injury, primarily cognitive symptoms, symptoms begin immediately after injury (no gradual or delayed onset), persistent disorientation, and confusion. Symptoms of PTSD that do not occur in TBI reexperiencing symptoms (e.g., flashbacks), and avoidance symptoms. [1]:323, [20]:280
Acute stress disorder (ASD) may occur immediately before PTSD, and the symptoms are similar. Acute Stress Disorder can only be diagnosed within a month of a traumatic event, and PTSD is only diagnosed if symptoms exist for longer than that. ASD is a risk factor for PTSD.
History of PTSD
Posttraumatic Stress Disorder first become an official diagnosis in 1980, when it was included in the Anxiety Disorders section of the DSM-III psychiatric manual.[32] Before 1980 the symptoms of Posttraumatic Stress was represented in both the DSM-I (in 1952) [33],[34] and the DSM-II (1968), and in medical literature under a variety of different names.[35], [39]
Friedman, M. J. (2013). Trauma and Stress-Related Disorders in DSM-5 (presentation used for expert training, ISTSS Conferences)
Lanius, R. A., Brand, B., Vermetten, E., Frewen, P. A., and Spiegel, D. (2012). doi:10.1002/da.21889 The dissociative subtype of posttraumatic stress disorder: rationale, clinical and neurobiological evidence, and implications. Depress Anxiety, 29(8) pp.701-708.
Meiser-Stedman R., Smith P., Glucksman E., Yule W., & Dalgleish T. (2008). The posttraumatic stress disorder diagnosis in preschool- and elementary school-age children exposed to motor vehicle accidents. Am J Psychiatry 165(10) pp.1326–1337. doi: 10.1176/appi.ajp.2008.07081282. PMID: 22431063.
Posluszny, D. M., Edwards, R. P., Dew, M. A., & Baum, A. (2011). Perceived threat and PTSD symptoms in women undergoing surgery for gynecologic cancer or benign conditions. Psychoncology, 20(7), pp.783-787. doi: 10.1002/pon.1771. PMID: 20878863.
Tedstone, J. E., & Tarrier, N. (2003). Posttraumatic stress disorder following medical illness and treatment. Clinical psychology review, 23(3), pp.409-448.
Wade, D., Hardy, R., Howell, D., & Mythen, M. (2013). Identifying clinical and acute psychological risk factors for PTSD after critical care: a systematic review. Minerva anestesiologica, 79(8), 944-963. PMID:23558761.
Wolf, E. J., Lunney, C. A., Miller, M. W., Resick, P. A., Friedman, M. J., & Schnurr, P. P. (2012). The dissociative subtype of PTSD: A replication and extension. Depression and Anxiety, 29, pp.679-688. doi: 10.1002/da.21946. http://onlinelibrary.wiley.com/doi/10.1002/da.21946/abstract
Taylor, S. (Ed). (2004). Advances in the treatment of posttraumatic stress disorder: Cognitive-behavioral perspectives. Springer Publishing Company.ISBN 0826120474.
Courtois, C. A. , Ford, J. D., Green, B. L., Alexander, P., Briere, J., Herman, J. L., Lanius, R., Stolbach, B. C., Spinazzola, J., Van der Kolk, B. A., Van der Hart, O. (2012). The ISTSS Expert Consensus Treatment Guidelines For Complex PTSD In Adults. Journal of Traumatic Stress, 24(6), pp. 615-627.
Dunmore, E. C.; Clark, D. M., Ehlers, A. (1997). Cognitive factors in persistent versus recovered post-traumatic stress disorder after physical or sexual assault: a pilot study. Behavioural and Cognitive Psychotherapy, 25, pp. 147–159.
Dunmore, E.C.; Clark, D. M., Ehlers, A. (1999). Cognitive factors involved in the onset and maintenance of posttraumatic stress disorder (PTSD) after physical or sexual assault. Behaviour Research and Therapy, 37, pp. 809–829. PMID: 10458046
Newman, E., Kaloupek, D. G., Keane, T. M. (1996) (coauthors: van der Kolk, B. A., McFarlane, A. C., Weisaeth, L. (Eds.)). Assessment of posttraumatic stress disorder in clinical and research settings. In Traumatic Stress the Effects of Overwhelming Experience on Mind, Body, and Society. New York:Guilford Publications.ISBN 1606238450.
American Psychiatric Association (1952). Diagnostic and Statistical Manual: Mental Disorders (DS). Washington, DC: American Psychiatric Association.
Blair Simpson, H. (2010) (coauthors: Neria, Y., Lewis-Fernández, R. (Eds)). Anxiety Disorders: Theory, Research and Clinical Perspectives. Cambridge Illustrated University Press. ISBN 1139490664.
Brett, E. A. (1996) (coauthors: van der Kolk, B. A., McFarlane, A. C., Weisaeth, L. (Eds.)). The classification of Posttraumatic stress disorder. In Traumatic Stress the Effects of Overwhelming Experience on Mind, Body, and Society. New York:Guilford Publications.ISBN 1606238450.
Murphy, S. A., Johnson, L. C., & Lohan, J. (2002). DURING THE FIRST 5 YEARS OF BEREAVEMENT. Journal of Loss & Trauma, 7(3), 203-222. doi: 10.1080/10811440290057620
Wright, A. A., Keating, N. L., Balboni, T. A., Matulonis, U. A., Block, S. D., & Prigerson, H. G. (2010). Place of death: correlations with quality of life of patients with cancer and predictors of bereaved caregivers' mental health. Journal of Clinical Oncology, 28(29), 4457–4464. doi: 10.1200/JCO.2009.26.3863. JCO-2009.

 Causes of PTSD: 10 common causes. Only a small percentage of people with PTSD are traumatized by combat. Source of data: Spence et al. (2011). PLoS ONE 6(7): e21864.
Causes of PTSD: 10 common causes. Only a small percentage of people with PTSD are traumatized by combat. Source of data: Spence et al. (2011). PLoS ONE 6(7): e21864.