Dissociative Identity Disorder (formerly Multiple Personality Disorder)
- Jump to:
- What is DID?
- Causes
- DSM 5 and ICD criteria
- Tests and Diagnosis
- Symptoms in the DSM-5
- Multiple Personality Disorder and DID
- Distinct Personality States/Alters
- Amnesia and Memory Lapses
- Treatment
- Is Integration Essential?
What is Dissociative Identity Disorder?
DID is:- a psychobiological response to traumas suffered in a specific time window in early childhood,
- a dissociative disorder, and
- a complex posttraumatic stress syndrome
How does DID develop?
- an important step in childhood development - the formation of a central, integrated consciousness - is impeded or prevented by repeated trauma
- the child uses radical denial and splitting to cope with the traumas, imagining that the traumas happened to "someone else"
- the child's fantasy capabilities and imagination give the different personality states their individual characteristics
- the extremely inconsistent and contradictory behavior of attachment figures and their denial of the trauma suffered by the child additionally foster the dissociative coping strategy. [19]:6-7

What is the cause?
Early childhood trauma causes Dissociative Identity Disorder to develop by preventing the child from forming a cohesive and fully integrated or unified sense of self, known as a core or fully integrated personality, during their earliest years. Instead of integrating into a core personality, people with DID experience prolonged trauma in early childhood which causes the original different "behavioral states" present from birth to become parts of the personality that are increasingly dissociated (disconnected) from each other, which prevents them from integrating to form a core personality. Over time, the early dissociated behavioral states, influenced by the trauma, develop into dissociative identities (also known as dissociative personality states,distinct personality states, alternate identities or alters). It is generally accepted that developing multiple identities protects the child psychologically by keeping trauma memories and emotions contained with specific identities, rather than overwhelming the child completely. [1]:122-123
Key Facts
- Dissociative Identity Disorder was previously called Multiple Personality Disorder (MPD), but has always been classified as a dissociative disorder; not a personality disorder. [3][5][6]
- Only around 6% of people with DID make their diagnosis obvious on an ongoing basis (R. P. Kluft, 2009). [1]
- Dissociative Identity Disorder is not rare, but relatively common, affecting around 1-3% of the population [1].
- Most people with DID have a mix of dissociative and posttraumatic symptoms, as well as non-trauma related symptoms.[2]
- Amnesia in people with DID can take many different forms, including amnesia for significant events in the past OR for events in everyday life. Amnesia is not limited to traumatic or stressful events. [4]:293
Is Multiple Personality Disorder the same as Dissociative Identity Disorder?
"it is a disorder characterized by the presence of two or more identities or personality states that recurrently take control of the individual's behavior accompanied by an inability to remember important personal information ... it is a disorder characterized by identity fragmentation rather than a proliferation of separate personalities" [24]:529
What is like to have DID?
DSM-5 Diagnostic Criteria
The most commonly guide used in psychiatry to diagnose mental disorders is the DSM-5, released by the APA in 2013.[3] The DSM-5 gives the following diagnostic criteria for Dissociative Identity Disorder:
Code 300.14
- "A. Disruption of identity characterized by two or more distinct personality states, which may be described in some cultures as an experience of possession. The disruption of marked discontinuity in sense of self and sense of agency, accompanied by related alterations in affect, behavior, consciousness, memory, perception, cognition, and/or sensory-motor functioning. These signs and symptoms may be observed by others or reported by the individual.
- B. Recurrent gaps in the recall of everyday events, important personal information, and/or traumatic events that are inconsistent with ordinary forgetting.
- C. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
- D. The disturbance is not a normal part of a broadly accepted cultural or religious practice. Note: In children, the symptoms are not better explained by imaginary playmates or other fantasy play.
- E. The symptoms are not attributable to the physiological effects of a substance (e.g., blackouts or chaotic behavior during alcohol intoxication) or another medical condition (e.g., complex partial seizures)." [3]:292
Differential Diagnosis
- Other Specified Dissociative Disorder (formerly Dissociative Disorder Not Otherwise Specified)
This can't occur alongside DID because it is only diagnosed when someone does not quite meet the DID criteria. The two most common forms of Other Specified Dissociative Disorder involve having amnesia and dissociative parts of your personality which are not quite distinct/separate enough for DID, and having dissociative parts which are distinct enough to be alter personalities but without amnesia between them. - Major Depressive Disorder (often just called "depression").
Depression is very common in people with DID, but both depressed mood and depressive thoughts fluctuate because they are present in some alters but not others. Because of this, Other specified depressive disorder may be diagnosed along with DID. [4]:296 - Bipolar Disorders - especially Bipolar II
Changes in mood occur in Dissociative Identity Disorder due to switching between alters (alters often have different mood states to each other). Bipolar II does not involve full-blown mania. - Posttraumatic Stress Disorder
There is now a dissociative subtype of PTSD and some overlapping features between DID and PTSD. PTSD is commonly comorbid with DID, but key differences exist as well. Complex PTSD is diagnosed as just PTSD in the DSM-5 (it is not considered a separate disorder). Differences between DID and Complex PTSD are described in the Dissociative Identity Disorder treatment guidelines for Adults; Complex PTSD is very common in people with Dissociative Identity Disorder, and dissociation is a symptom of both. - Psychotic Disorders (including Schizophrenia).
Hearing voices (which come from alter personalities), and symptoms of partial flashbacks like feeling touched when nobody is there may be mistaken for psychotic hallucinations. The passive influence of alters causes many psychotic-like symptoms, but without any loss of contact with reality. - Personality Disorders (especially Borderline Personality Disorder (BPD).
BPD has both transient stress-related dissociative symptoms and identity disturbance within its diagnostic criteria). Psychological tests can be used to determine if Dissociative Identity Disorder is present, and whether a personality disorder is also present. Self-injury and self-destructive behavior is also common in both DID and BPD. [1]:129, 137 - Substance/medication-induced disorders (e.g., Alcohol or drug addiction or side effects of another drug)
Certain substances can cause episodes of amnesia and altered behavior (e.g. alcohol) or other dissociative experiences - in DID these occur during times when no substance has been used. Substance use disorders are common in people with DID. [4]:297-298 - Conversion Disorder (Functional Neurological Symptom Disorder).
These disorders are common in people with DID, particularly psychogenic non-epileptic seizures (PNES), which can cause amnesia during the seizure only. [4]:297-298 - Seizure Disorders - especially Complex Partial Seizures.
EEG tests can differentiate between seizure disorders and seizure-like symptoms in DID. Dissociative symptoms are far greater in people with DID. [4]:297 - Factitious Disorder and Malingering
Both of which involve intentionally and knowingly pretending to have DID, e.g., by repeatedly giving false information to professionals. This is very different to having doubts about symptoms, or wondering if you 'made it all up'. Psychological tests, observation, and corroborating history can be used to help diagnose. [3]:296-297 Malingerers have a clear motive, e.g. to avoid responsibility for a crime (despite the fact the diagnosis is rarely accepted for an 'insanity' defense).
Symptoms in the DSM-5
Dissociative Identity Disorder has a wide variety of symptoms, the primary symptoms that occur in all people with DID are described in the DSM psychiatric manual. The key characteristic of Dissociative Identity Disorder is the presence of at least two distinct personality states (described in some cultures as an experience of "possession"). The presence of reoccurring periods of amnesia is the next most important characteristic, sometimes referred to as recurrent lapses in memory which go beyond ordinary forgetting. [3]:291-292 The remaining diagnostic criteria require symptoms to cause distress and/or impaired functioning in at least one area of life, and state that DID can only be diagnosed if no other condition provides a better explanation for symptoms. A mix of secondary symptoms are found in DID, particularly those caused by the passive influence of alters intruding into awareness, but no single secondary symptom is present in everyone with Dissociative Identity Disorder, and these do not form part of the diagnostic criteria.
Distinct Personality States
A person with Dissociative Identity Disorder has "distinct personality states", this phrase refers to distinct (different, separate) identities that feel, think and behave as if they were different personalities, they are often called alternate personalities, alternate identities, or "alters". Other terms sometimes used instead of "alters" include dissociative parts (of the personality), Apparently Normal Part of the personality (ANP), and Emotional Part of the personality (EP).[1], [4]:193 Alters are only overt (obvious) in a small minority of people with DID in clinical situations. A change introduced in the DSM-5 makes it possible to diagnose DID without the diagnosing clinician directly observing a switch between alters: instead, DID can be diagnosed if the person self-reports their presence and effects, or if another person describes observing a switch between alters. Two clusters of symptoms indicate the presence of alters if they are not observed, these are described in the DSM-5's extended description of Dissociative Identity Disorder:
- Sudden alterations or discontinuities in sense of self and sense of agency (Criteria A),
- and recurrent episodes of dissociative amnesia (Criteria B). [3]:291-292
Sense of Self and Agency
The terms "sense of self" and "sense of agency" are used in the DSM's Dissociative Identity Disorder Criterion A, which describes the presence of distinct personality states, better known as alter personalities. It is the discontinuities (switches) between alters, as well as their presence, that this criterion describes.
A discontinuity in a person's sense of self can affect any part of someone's functioning. Attitudes, outlooks and personal preferences like preferred foods or clothes may change suddenly and inexplicably, and then change back again. This happens because alter personalities have different attitudes, outlooks and preferences, so a very sudden change without explanation occurs when an alter has either taken control or is strongly influencing the person. When that alter is no longer active, everything changes back (until the next time the same alter is active). During these times, a person may find have bought clothes they would never choose to wear, or a very outgoing person may suddenly become shy and introverted with no apparent reason.
Discontinuity in a person's sense of agency means not feeling in control of, or as if you don't "own" your feelings, thoughts or actions. For example, experiencing thoughts, feelings or actions that seem as if they are "not mine" or belong to someone else. This is not the delusional belief that they belong to an outside person, it is the perception that their own speech, thoughts, and/or behavior do not feel like they belong to them and may make no sense to them. Emotions and impulses are often described as puzzling to the person. This happens in Dissociative Identity Disorder because some of the thoughts, feelings or actions of alter personalities intrude into their conscious awareness, even when they are not aware they have any alter personalities, or have amnesia for their actions.[3]:298 This is known as passive influence or partially dissociated intrusions of alter identities into conscious awareness (see below).
- I have no control, I watch what happens, but can't stop it [3]:293
- I find myself "coming to" in the downtown area where I live, but I won't remember where I parked the car [14]:63
- I have found myself crying uncontrollably and sucking my thumb, but I can't explain why [14]:63
- Sometimes I've had people call me by a name I don't recognize, and I don't know who they are [14]:15
A similar depersonalized experience can happen briefly during times of severe stress, especially in people with Borderline Personality Disorder, except that the person perceives the behavior as "out of character" rather than like being a totally different person (egodystonic). In Dissociative Identity Disorder, there may no obvious stressor or trigger causing the switch in personality state, the actions and words spoken may not relate to any prior distress, and the duration can be considerably longer (hours, days, or more). In DID, this happens because an alter personality has taken executive control, so attitudes, outlook and personal preferences change at the same time - leaving a feeling as if someone else is in control of their body. This change in control is known as switching, only in Dissociative Identity Disorder or similar forms of Other Specified Dissociative Disorder can a person switch to an alter personality, because no other diagnosis has alter personalities that control (of the body) can be switched to.
Rapidly switching moods (within minutes or hours) are commonly caused by the presence of alters which have different moods, these changes in moods can be puzzling and lead to a misdiagnosis of Bipolar Disorder, type 2, however mood changes in Bipolar Disorder do not switch back and forth as rapidly, with rapid-cycling bipolar involving several switches per year only.[3]:296
The combined changes in "sense of self" and "sense of agency" can cause a person to find themselves feeling like they are watching passively while someone else controls their body; they hear themselves speaking words they would never normally speak and that may not make sense to them, and which they are powerless to stop. The person has become a depersonalized observer of themselves.
Some people describe this combined change of "sense of self" and "sense of agency" as feeling like an experience of possession, in a non-religious sense, or having their body "hijacked". A person with DID may find that their body feels totally different during this time (e.g., like a small child, the opposite gender, huge and muscular), or may feel as if they are suddenly younger or older.[3]:298
Recurrent Amnesia: Criterion B
Several different types of amnesia can occur in people with Dissociative Identity Disorder, the common types are:
- "gaps in past memory of personal life events" (e.g., periods of childhood or adolescence; some important life events, such as the death of a grandparent, getting married, giving birth); this amnesia does not need to be restricted to traumatic events
- "lapses in dependable memory" (e.g., of what happened today, remembering how to do well-learned skills like how to do their job, drive, read, etc.); this refers to the whole person - for example having a child alter who does not know how to read would prevent the person from remembering how to read when that alter was in control of the body
- "discovery of evidence of their everyday actions and tasks that they do not recollect doing" (e.g., finding unexplained objects in their shopping bags or among their possessions; finding perplexing writings or drawings that they must have created; discovering injuries; "coming to" in the midst of doing something). Dissociative fugues, which involve travel to an unusual place without any memory of the journey or its purpose, are common. People find suddenly find themselves "coming to" at the beach, hiding in a closet at home, in a nightclub, or in bed without any memory of the "lost" time. [3]:293
Passive Influence of Alters
The passive influence of alters cause many common secondary symptoms in Dissociative Identity Disorder, symptoms that are often described as confusing and frightening, and can make a person feel like they are going crazy.[17]:8 People with DID normally have some of these symptoms, but all of them are optional rather than needed for diagnosis. While none of these symptoms are unique to Dissociative Identity Disorder, understanding why they happen and that they are common in DID can be very helpful.
Examples of passive influences:
- Hearing a child's voice - when no child is visible
- Speech insertion - saying things you don't remember saying, or didn't intend to say
- Thought insertion* - strong thoughts seem to come out of nowhere and don't feel like yours
- Thought withdrawal* - your thoughts may suddenly seem to get taken away
- Internal conversations or hearing voices arguing*, internal struggle
- Hearing voices that are threatening, harsh or tell you to do self-destructive acts
- Intrusive or “made” feelings or emotions* - unexpected surges of feelings that are puzzling
- Intrusive or “made” impulses or “made” actions* - some impulses or behavior doesn't feel like yours, you may be or may not be fully aware of it at the time, you may be told of things you did by other people, or find you have self-injured
- Temporary loss of well rehearsed knowledge or skills, e.g. forgetting where you live or how to drive or do your job (amnesia)
- Self-alteration - suddenly, inexplicably feeling that your body, thoughts, or urges belong to someone else or are not yours (when not feeling depersonalized/detached from self, that occurs without switching to an alter)
- Self-puzzlement - you don't understand why you feel and behave as you do [17]:4, 14, [18]:231-232
The symptoms marked with * are known as Schneider's first-rank symptoms (FRS) and were historically used to diagnose Schizophrenia, but are actually more common in DID. People with DID do not given them delusional explanations, because they are not experiencing a psychotic symptom (except in the uncommon case that a psychotic disorder also exists). Schizophrenia is a very common misdiagnosis for DID.
An influential study of 220 people with Dissociative Identity Disorder found that most people experienced several of the symptoms above, although no single symptom was experienced by everyone, and none are actually diagnostic criteria. These symptoms can be understood as the result of alter personalities partially intruding into a person's conscious awareness.[17]:8, 14 For example, hearing a child's voice can be caused by the voice of a very young alter personality intruding into conscious awareness without fully taking over control.
ICD-11 Diagnostic Criteria
Code 6B64
- "Disruption of identity characterized by the presence of two or more distinct personality states (dissociative identities), involving marked discontinuities in the sense of self and agency. Each personality state includes its own pattern of experiencing, perceiving, conceiving, and relating to self, the body, and the environment.
- At least two distinct personality states recurrently take executive control of the individual’s consciousness and functioning in interacting with others or with the environment, such as in the performance of specific aspects of daily life (e.g., parenting, work), or in response to specific situations (e.g., those that are perceived as threatening).
- Changes in personality state are accompanied by related alterations in sensation, perception, affect, cognition, memory, motor control, and behaviour. There are typically episodes of amnesia inconsistent with ordinary forgetting, which may be severe.
- The symptoms are not better accounted for by another mental disorder (e.g., Schizophrenia or Other Primary Psychotic Disorder).
- The symptoms are not due to the effects of a substance or medication on the central nervous system, including withdrawal effects (e.g., blackouts or chaotic behaviour during substance intoxication), and are not due to a Disease of the Nervous System (e.g., complex partial seizures) or to a Sleep-Wake disorder (e.g., symptoms occur during hypnagogic or hypnopompic states).
- The symptoms result in significant impairment in personal, family, social, educational, occupational or other important areas of functioning. If functioning is maintained, it is only through significant additional effort." [6]
- "Alternation between distinct personality states is not always associated with amnesia. That is, one personality state may have awareness and recollection of the activities of another personality state during a particular episode. However, substantial episodes of amnesia are typically present at some point during the course of the disorder.
- In individuals with Dissociative Identity Disorder, it is common for one personality state to be ‘intruded upon’ by aspects of other non-dominant, alternate personality states without their taking executive control, as in Partial Dissociative Identity Disorder. These intrusions may involve a range of features, including cognitive (intruding thoughts), affective (intruding affects such as fear, anger, or shame), perceptual (e.g., intruding voices or fleeting visual perceptions), sensory (e.g., intruding sensations such as being touched, pain, or altered perceived size of the body or of part of the body), motor (e.g., involuntary movements of an arm and hand), and behavioural (e.g., an action that lacks a sense of agency or ownership). The personality state that is intruded upon in this way commonly experiences the intrusions as aversive, and may or may not realize that the intrusions relate to features of other personality states."
- Dissociative Identity Disorder is commonly associated with serious or chronic traumatic life events, including physical, sexual, or emotional abuse." [6]
ICD-11 Description
"Dissociative identity disorder is characterised by disruption of identity in which there are two or more distinct personality states (dissociative identities) associated with marked discontinuities in the sense of self and agency. Each personality state includes its own pattern of experiencing, perceiving, conceiving, and relating to self, the body, and the environment. At least two distinct personality states recurrently take executive control of the individual’s consciousness and functioning in interacting with others or with the environment, such as in the performance of specific aspects of daily life such as parenting, or work, or in response to specific situations (e.g., those that are perceived as threatening). Changes in personality state are accompanied by related alterations in sensation, perception, affect, cognition, memory, motor control, and behaviour. There are typically episodes of amnesia, which may be severe. The symptoms are not better explained by another mental, behavioural or neurodevelopmental disorder and are not due to the direct effects of a substance or medication on the central nervous system, including withdrawal effects, and are not due to a disease of the nervous system or a sleep-wake disorder. The symptoms result in significant impairment in personal, family, social, educational, occupational or other important areas of functioning." [6]
Alternative names:- Multiple Personality
- Multiple Personality Disorder [6]
ICD-11 Differential Diagnosis
- Trance Disorder and Possession Trance Disorder
- Partial Dissociative Identity Disorder (P-DID)
- Other Dissociative Disorders
- Schizophrenia or Other Primary Psychotic Disorders
- Post-Traumatic Stress Disorder (PTSD) and Complex Post-Traumatic Stress Disorder (C-PTSD)
- Obsessive-Compulsive Disorder (OCD)
- Personality Disorder [6]
Additional information
The ICD-11 provides a variety of additional information about DID.[6]Changes from the ICD-10 to ICD-11 for DID
Several significant changes have been made, including recognizing each alter identity/distinct personality state is not a complete personality but a dissociated part of a single personality. It also recognizes that some alters may be partially integrated with each other, for example co-consciousness (sharing memories in the present), with amnesia being typical but not essential.[6] The ICD 11 states that at least two identities must be able to physically take control e.g. either act in daily life, or in response to specific situations The name has also changed from Multiple Personality Disorder to Dissociative Identity Disorder, it has been given greater prominence and is not longer a subtype of other dissociative disorders. The ICD-11 has also removed the previous speculation that DID might be iatrongenic (a negative result of prior drugs or treatment).[5], [6] A new diagnosis of Partial Dissociative Identity Disorder has been created, which is equivalent to the most common type of Other Specified Dissociative Identity Disorder in the DSM-5 (informally known as OSDD-1a).[32]
ICD-10 Diagnostic Criteria (retired)
Code F44.81In the World Health Organization's ICD-10 diagnostic manual, Dissociative Identity Disorder is still referred to as Multiple Personality, and classified as one of several Other dissociative [conversion] disorders within code F44.8. The diagnostic criteria are:
- "A. The existence of two or more distinct personalities within the individual, only one being evident at a time.
- B. Each personality has its own memories, preferences and behaviour patterns, and at some time (and recurrently) takes full control of the individual's behaviour.
- C. Inability to recall important personal information, too extensive to be explained by ordinary forgetfulness.
- D. Not due to organic mental disorders (F0) (e.g. in epileptic disorders) or psychoactive substance-related disorders (F1) (e.g. intoxication or withdrawal).
- E. The symptoms are not attributable to the physiological effects of a substance (e.g., blackouts or chaotic behavior during alcohol intoxication) or another medical condition (e.g., complex partial seizures)." [5]:123
Diagnostic Tests and Interviews
- The Dissociative Experiences Scale (DES) is a self-assessment screening tool (a questionnaire) that is useful for identifying people who experience a high degree of dissociation. It is available in many languages. A definite diagnosis should only be made by a qualified clinician. This can be done using a clinical interview based on the Dissociative Experiences Scale, or by using one of the two clinical interviews developed for Dissociative Disorders, the SCID-D or DDIS (described below). [1]:126-127,[11]:21, [12], [14]
- The Somatoform Dissociation Questionnaire (SDQ-20) is another self-assessment screening tool for Dissociative Identity Disorder and other Dissociative Disorders. [1]:127 It is a questionnaire that measures physical symptoms historically found to be common in people with Dissociative Disorders, including DID and Other Specified Dissociative Disorder. Symptoms assessed include sensory disturbances (e.g., tunnel vision, psychogenic blindness, auditory distancing, numbness/insensitivity to pain), other conversion disorder symptoms (e.g., psychogenic paralysis and non-epileptic seizures), genital symptoms (difficulty urinating, genital pain that does not occur during intercourse), and more.[1]:127, [28] The SDQ-20 was developed Dutch clinicians and researchers in the late 1990s. [1]:127 Average scores have been published for the DID, OSDD (formerly known as DDNOS), Somatoform Disorders, Eating Disorders, Schizophrenia, Anxiety Disorders, major Depression, mixed psychiatric disorders, Bipolar disorder, and a non-psychiatric group. [7]:25 The SDQ-20, and the shorter SDQ-5, are available online in multiple languages, along with their scoring instructions. [7]:36 Somatoform Dissociation is "manifested in the loss of the normal integration of somatoform components of experience, bodily reactions and functions ... it is a disturbance of mental function". [29] This has been shown to be higher in Dissociative Identity Disorder than in people from any other diagnostic group, including those diagnosed with Somatoform Disorders, and it also correlates with trauma history, especially physical and sexual trauma occurring from ages 0-6 (both self-reported and corroborated trauma).[29]:722, [30]:25
- Dissociative Disorders Interview Schedule (DDIS), developed by Dr Colin A. Ross et al.[13] This uses some observation from a clinician, and is a structured interview. No special training is needed to carry this out, and it can be downloaded without charge from the Ross Institute. The DDIS has been updated for the DSM-5. [13]
- Structured Clinical Interview for Dissociative Disorders (SCID-D) is regarded as the gold-standard interview for diagnosing Dissociative Identity Disorder, Other Specified Dissociative Disorder and all other Dissociative Disorders. [15]:102 It is a semi-structured clinical interview that uses observation from a trained clinician. It was developed primarily by Dr Marlene Steinberg and can accurately assess all Dissociative Disorders.[12], [14] It can distinguish between all Dissociative Disorders and dissociative or identity symptoms present in Borderline Personality Disorder, Schizophrenia, PTSD, major Depression, and Acute Stress Disorder. Each domain of dissociative symptoms is assessed: amnesia, depersonalization, derealization, identity confusion and identity alteration, and then rated for severity (absent, mild, moderate, or severe). This interview can only be carried out after specific training, and includes the interviewer noting subtle indicators of dissociation, including intra-interview amnesia, also known as micro-amnesias, eye movements, trance states, changes in demeanor and mood, avoidance or uncertainty in answering certain questions. [14]:80,148 The questions are open-ended to elicit detailed answers. Questions avoid "leading or intrusive" wording, but many people may still have emotional reactions to certain questions. [14]:80, 148
Clinicians wishing to use the SCID-D can receive training from International Society for the Study of Trauma and Dissociation (ISSTD), or affiliate organizations worldwide. The SCID-D interview has been updated for use with both the DSM-5 and the ICD-11 diagnostic criteria, and the participant interview packs completed by clincians are available from American Psychiatric Association Publishing. [33] - The Multidimensional Inventory of Dissociation (MID), a comprehensive tool based on a combination of self-report and clinical judgementalso exists.[1]:126, [15] The MID ignores normal experiences of dissociation, and assesses only pathological dissociation, it is only available to clinicians, who can request a copy from author Paul F. Dell. The MID can reliably help a clinican diagnose Dissociative Identity Disorder and Other Specified Dissociative Disorder (DDNOS), and identify PTSD symptoms and problematic Borderline Personality Disorder traits. It includes over 200 questions, and produces a series of graphs and total scores for different aspects of dissociation, from which a clinician judgement is made. [15]
Treatment
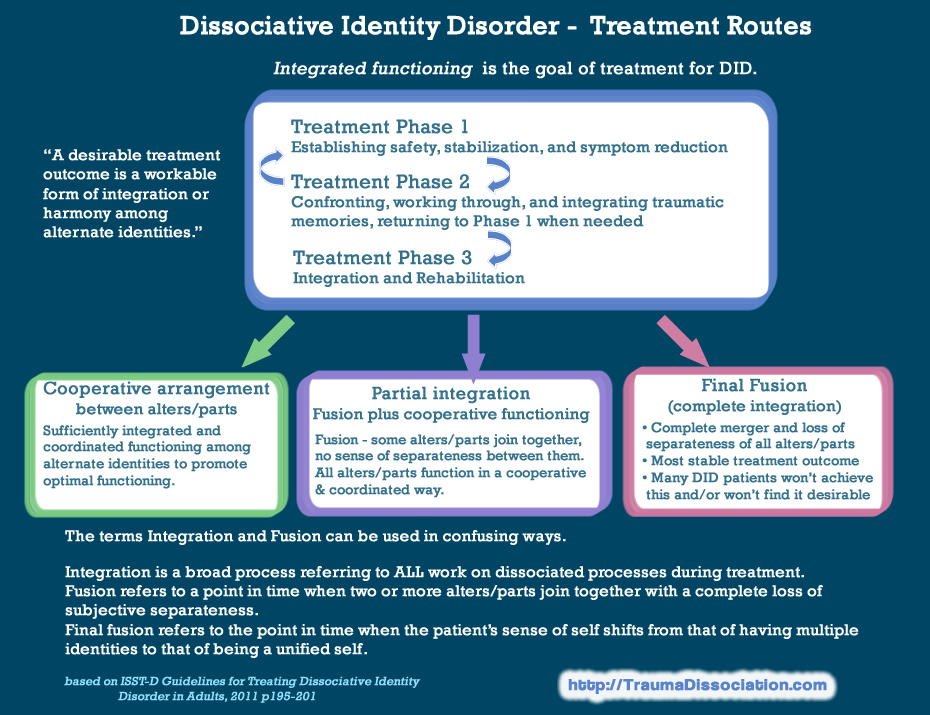
The ISST-D Treatment Guidelines for Dissociative Identity Disorder, which also cover similar forms of Other Specified Dissociative Disorder (OSDD-1) or Partial Dissociative Identity Disorder (P-DID), describe how to diagnose and treat DID, including specific therapy techniques and the use of off-label medications. [1] A three phase treatment approach is recommended for DID/OSDD-1, based on the Complex PTSD treatment guidelines. The treatment guidelines for DID, which were first published over 20 years ago, were developed by expert consensus and guided by large-scale clinical research. The current adult treatment guideline, from 2011, is free to download from the International Society for the Study of Trauma and Dissociation, and there is a different version for DID and dissociative symptoms in children and adolescents. [1], [3]
Research shows that treatment based on the DID treatment guidelines, which follow the general principles of psychotherapy and focuses primarily on outpatient psychotherapy, improves symptoms while increasing functioning, and reducing rates of intentional self-injury and hospitalization. [1], [9]:169 Poor outcomes were found when DID treatment did not follow the guidelines, for example treatment which did not directly engage alter identities and seek to reduce amnesia, [9]:169 or when treatment was instead focused on "memory recovery". [9]:180 Harm is far more likely to occur when DID was not treated at all. [9]:169 Treating Dissociative Identity Disorder did not only consistently improve dissociative symptoms, it also improved patients' general distress and depression. [9]:175
Psychotherapy
Long-term psychotherapy following the ISST-D treatment guidelines is the primary method of treatment for Dissociative Identity Disorder, and evidence-based research shows patients make significant improvements when psychotherapy adheres to the treatment guidelines. No specific type of therapy is recommended, although if hypnotherapy / hynosis is used, it should not be used to attempt to retrieve dissociated memories, and a higher level of training is needed to perform EMDR (Eye Movement Desensitization and Reprocessing) with DID/OSDD patients to avoid a flooding or trauma memories or otherwise destabilising the person. [1], [9] Psychotherapy for Dissociative Identity Disorder follows the basic principles of general psychotherapy, [1] with additional of techniques which address dissociative symptoms, [1] including working directly with alters or dissociative parts rather than telling them to go "back inside". Treating Dissociative Identity Disorder is not primarily based around uncovering trauma memories, processing trauma, hypnotism, or trauma exposure techniques. A recent study that compared experts in the treatment of Dissociative Disorders to community clinicans found that experts spent more time on techniques for the containment of trauma memories than uncovering them.[8]:4 Experts in treating DID also spent more time on grounding and safety interventions, although treatment that is entirely limited to skills training to reduce dissociation is known to be ineffective. [1], [8]:4Progress through the three recommended treatment stages is explained:
Is Integration Essential?
Integration in DID refers to the process of someone gradually getting closer and more connected to other parts of themselves, so that alter identities are not as dissociated (disconnected) from the person, or from each other. [1]:133 Many people use the word integration to refer solely to fusion, which is the permanent merging of alters within a person with Dissociative Identity Disorder. The full integration of alters into a single identity, known as final fusion or unification, is not essential for healing to take place: it only a later part of a long-term process, with many improvements in daily life and reductions in distress occurring on the way.[1]:132-134 Some people are never being able to fully integrate, and others decide to choose an resolution as an alternative treatment goal. [1]:132 Some people mistakenly believe that the only goal of treatment for Dissociative Identity Disorder is simply to have a single identity rather than multiple identities, however, this simplistic view does not take into the improvements from the work of addressing the traumatic experiences that caused multiple identities in the first place, the degree of distress or impairment, or recovery from the other co-morbid disorders that people with DID typically have. Resolution, which is integrated functioning, achieving a workable form of integration or harmony among identities, is a common alternative treatment goal. [1]:132-134 While some people do choose final fusion as their goal, and this outcome is seen by some professionals (e.g., Kluft), as the most stable over the longer term, not everyone wants to achieve this, and some adults find they are not able to fully achieve this.[1]:132 Reasons for not integrating fully include serious and long-term situational stress, avoiding addressing unresolved and painful life issues or traumatic memories, lack of money for treatment, comorbid physical or mental disorders which don't improve as treatment progresses, advanced age, and/or significant investment in either alters themselves or in having DID. [1]:133-134 Children and adolescents with DID are able to achieve final fusion much more quickly, and this is the recommended treatment goal for them. [13]
Resolution
An alternative treatment goal for adults with DID, as described by the ISST-D treatment guidelines, involves achieving a workable form of harmony between alter identities, known as a cooperative arrangement or resolution, and this is actually a more common outcome than full integration.[1]:133 Resolution involves achieving a cooperative arrangement between the person's identities, which need to be sufficiently integrated (connected) and have a co-ordinated way of functioning that promotes "optimal functioning", [1]:132-134 this is sometimes described as healthy or functional multiplicity.[14] International treatment studies have shown that long-term psychotherapy helps people with Dissociative Identity Disorder achieve significant and sustainable improvements in their overall mental health as well as their DID symptoms, regardless of whether they eventually reach final fusion, and whether they are treated by a Dissociative Disorders specialist or a "community clinician".
Functional Multiplicity
Healthy multiplicity also known as functional multiplicity, is achieved when a person has multiple, distinct identities, but does not have clinically significant distress or impairment as a result of their dissociative identities. [14] A person who meets all the diagnostic criteria for Dissociative Identity Disorder except Criteria C (distress or impaired functioning in a major area of life) may be referred to as a healthy multiple, or less commonly as a healthy plural, and does not have any dissociative disorder since all of them require significant distress or impaired functioning.[4], [6] The presence of alters and amnesia alone is not enough to classify someone as having Dissociative Identity Disorder or a "mental disorder": there are more than two diagnostic criteria. [3], [6]
Note: The international treatment guidelines for Dissociative Identity Disorder in Adults state that therapists should not try to ignore or "get rid" of any alters: integration involves merging/fusing together, which is the opposite. Previous treatment studies have shown full integration (final fusion) was achieved for between 1 in 3 and 1 in 6 of people, but do not generally state how many people chose not to fully integrate.
See also: Healthy Multiplicity
Medication and DID
Although psychotropic (psychiatric) medication is not a primary treatment for complex dissociative disorders, most DID patients do take some form of medication. This typically targets the comorbid conditions, including PTSD, mood disorders (e.g., depression), and any obsessive-compulsive symptoms.[1] The use of anti-depressants is particularly common. People with DID or other complex posttraumatic conditions may only partially respond to medication, in DID there is the further complication of potential amnesia for whether other alters have refused to take medication or taken too much. The DID treatment guidelines for adults state that alters may report different responses to the same medication, possibly due to physiological differences, physical symptoms which have a psychological cause (somatoform symptoms), and/or the alters' experience of separateness.[1]
History of DID
Dissociative Identity Disorder is sometimes incorrectly believed to be a "new" diagnosis, but it has a long history of recognition, and has been part of the Diagnostic and Statistical Manual for Mental Disorders since its first edition was published in 1952.[21] Before this, Dissociative Identity Disorder was also described in earlier diagnostic manuals,[22],[23]:377,[26] and for hundreds of years in books and writing, including those by many famous "physicians" and scientists including Sigmund Freud, Pierre Janet, and Morton Prince (founder of the Journal of Abnormal Psychology). Dissociative Identity Disorder has retained the same diagnostic code, DSM code 300.14, for almost 50 years.[3],[22-24]
Historical Names for Dissociative Identity Disorder
The history of Dissociative Identity Disorder in diagnostic manuals parallels that of Posttraumatic Stress Disorder, with both becoming a separate diagnosis with the publication of the DSM-III in 1980. DID has historically been described alongside other Dissociative Disorders, including Amnesia, Fugue and Depersonalization, which are not subject to suggestions that they are either a "new" or "controversial" diagnosis.
- Hysteria - Statistical Manual for the Use of Institutions for the Insane, 1918 (Grob, p.426)
- Dissociated Personality - DSM-I, 1952
- Hysterical neurosis, dissociative type - DSM-II, 1968 - "multiple personality" listed as a symptom
- Multiple Personality - DSM-III, 1980
- Multiple Personality Disorder - DSM-III-R, 1987
- Dissociative Identity Disorder (Multiple Personality Disorder) - DSM-IV, 1994
- Dissociative Identity Disorder - DSM-5, 2013
DSM-I (1952): Dissociated personality. Code 000-x02
"Dissociative reaction
This reaction represents a type of gross personality disorganization, the basis of which is a neurotic disturbance, although the diffuse dissociation seen in some casts may occasionally appear psychotic. The personality disorganization may result in aimless running or "freezing." The repressed impulse giving rise to the anxiety may be discharged by, or deflected into, various symptomatic expressions, such as depersonalization, dissociated personality, stupor, fugue, amnesia, dream state, somnambulism, etc. The diagnosis will specify symptomatic manifestations. These reactions must be differentiated from schizoid personality, from schizophrenic reaction, and from analogous symptoms in some other types of neurotic reactions. Formerly, this reaction has been classified as a type of "conversion hysteria". [21]:34
DSM-II (1968): Hysterical neurosis, dissociative type. Code 300.14
300.1 Hysterical neurosis
This neurosis is characterized by an involuntary psychogenic loss or disorder of function. Symptoms characteristically begin and end suddenly in emotionally charged situations and are symbolic of the underlying conflicts. Often they can be modified by suggestion alone. This is a new diagnosis that encompasses the former diagnoses "Conversion reaction" and "Dissociative reaction" in DSM-I. This distinction between conversion and dissociative reactions should be preserved by using one of the following diagnoses whenever possible.
300.14 Hysterical neurosis, dissociative type
"In the dissociative type, alterations may occur in the patient's state of consciousness or in his identity, to produce such symptoms as amnesia, somnambulism, fugue, and multiple personality." [22]:40
DSM-III (1980): Multiple Personality. Code 300.14
This version of the DSM was the first to include diagnostic critera for mental disorders, rather than only a description. Other changes in this update include moving all Dissociative Disorders to a new section, renaming Traumatic Neurosis to PTSD, and changing it to a separate diagnosis. The description of Dissociative Identity Disorder covers two pages, ending with these criteria:
"A. The existence within the individual of two or more distinct personalities, each of which is dominant at a particular time.
B. The personality that is dominant at any particular time determines the individual's behavior.
C. Each individual personality is complex and integrated with its own unique behavior patterns and social relationships". [23]:259
The role of childhood trauma was recognized as follows: "Onset of Multiple Personality may be in early childhood or later. The disorder is rarely diagnosed until adolescence," and "Child abuse and other forms of severe emotional trauma in childhood may be predisposing factors." It was recognized as more common in females, with diagnosis commonly occurring in late adolescence, or young adult females.
Differences between alter personalities mentioned included reports of "being of the opposite sex, of a different race or age, or from a different family than the original personality," and that they may have different responses to "physiological and psychological measurements". The diagnosis was described as "apparently extremely rare".[23]:257-258
The description stated that each personality had "unique memories, behavior patterns, and social relationships . . ." and that switches between identities were "sudden and often associated with psychosocial stress". Limited amnesia and a typical lack of awareness of alter personalities was described:
"Usually the original personality has no knowledge or awareness of the existence of any of the other personalities (subpersonalities). When there are more than two subpersonalities in one individual, each is aware of the others to varying degrees. The subpersonalities may not know each other or be constant companions. At any given moment one personality will interact verbally with the external environment, but none or any number of the other personalities may actively perceive (i.e., "listen in on”) all that is going on." [23]:257-259
The disorder was recognized as not occurring alone, with medically unexplained physical symptoms being common (diagnosed as Somatoform Disorders), as well as "Psychological Factors Affecting Physical Condition". Differential Diagnosis are listed as Psychogenic Amnesia, Psychogenic Fugue, and Psychotic Disorders, e.g., Schizophrenia spectrum disorders, plus Malingering (intentionally faking illness for an obvious gain).[23]:257-259
DSM-III-R (1987): Multiple Personality Disorder. Code 300.14
Multiple Personality officially became Multiple Personality Disorder in 1987; other changes included recognizing self-injury, self-harm, and addiction to medication as common in people with MPD, and adding Borderline Personality Disorder as a differential diagnosis. The diagnostic criteria are given below.
"A. The existence within the person of two or more distinct personalities or personality states (each with its own relatively enduring pattern of perceiving, relating to, and thinking about the environment and self.
B. At least two of these personalities or personality states recurrently take full control of the person's behavior." [20]:41, [27]:272
The term 'personality" is defined for the first time, and "personality state" is introduced:
The essential feature of this disorder is the existence within the person of two or more distinct personalities or personality states. Personality is here defined as a relatively enduring pattern of perceiving, relating to, and thinking about the environment and one’s self that is exhibited in a wide range of important social and personal contexts.
Personality states differ only in that the pattern is not exhibited in as wide a range of contexts. In classic cases, there are at least two fully developed personalities; in other cases, there may be only one distinct personality and one or more personality states. In classic cases, the personalities and personality states each have unique memories, behavior patterns, and social relationships; in other cases, there may be varying degrees of sharing of memories and commonalities in behavior or social relationships.[27]:269
DSM-IV (1994): Dissociative Identity Disorder. Code 300.14
"A. The presence of two or more distinct identities or personality states (each with its own relatively enduring pattern of perceiving, relating to, and thinking about the environment and self).
B. At least two of these identities or personality states recurrently take control of the person's behavior.
C. Inability to recall important personal information that is too extensive to be explained by ordinary forgetfulness.
D. The disturbance is not due to the direct physiological effects of a substance (e.g., blackouts or chaotic behavior during Alcohol Intoxication) or a general medical condition (e.g., complex partial seizures). NOTE: In children, the symptoms are not attributable to imaginary playmates or other fantasy play." [24]:529
DSM-5 (2013): Dissociative Identity Disorder. Code 300.14
Several changes were made, including adding a new criteria:
"The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning."
This changes means that a person who has alter identities (and some amnesia), is no longer automatically considered to have a mental health disorder. A person can only be diagnosed if they experiences distress or difficulties in life as a result.
See DSM-5 criteria. [3]
External links
- Guidelines For Treating Dissociative Identity Disorder In Adults (2011) - International Society for the Study of Trauma and Dissociation
- Guidelines for the Evaluation and Treatment of Dissociative Symptoms in Children and Adolescents (2003) - International Society for the Study of Trauma and Dissociation
- Multidimensional Inventory of Dissociation diagnostic tool

