Other Disorders: Trauma-related Disorders and Misdiagnosis
Misdiagnosis and Differential Diagnosis
Posttraumatic Stress Disorder
Many differential (alternative) diagnoses exist, including Adjustment Disorders, and Acute Stress Disorder, which has a shorter duration (under a month), Anxiety disorders and Obsessive-compulsive disorder (OCD), Major depressive disorder, Dissociative Disorders and Personality Disorders. Interpersonal difficulties which begin or were greatly increased, after a traumatic event may indicate PTSD since a personality disorder would have these difficulties independently of whether any trauma occurred. Flashbacks in PTSD need to be distinguished from the illusions and hallucinations present in schizophrenia and other psychotic disorder. [2]
Acute Stress Disorder
Adjustment Disorders, Panic Disorder, Dissociative Disorders, Posttraumatic Stress Disorder, Obsessive-compulsive disorder (OCD), Psychotic Disorders and Traumatic Brain Injury are other diagnoses which could be considered.
Adjustment Disorders
Major Depressive Disorder (depression), Acute Stress Disorder or PTSD and Personality Disorders can be considered as alternative diagnoses, as well as normal stress reactions. [2]
Dissociative Identity Disorder
Bipolar Disorder involves changes in mood that cycle between Depression and either mania (or the less severe hypomania), and sometimes "mixed episodes" which have features of both. In Dissociative Identity Disorder there are also frequent mood changes, these rapidly switching moods (within minutes or hours) are commonly caused by the presence of alters which have different moods, and the changes in moods can be puzzling to the person. The common misdiagnosis is Bipolar Disorder type 2, which involves hypomania rather than full mania, however mood changes in Bipolar Disorder do not switch back and forth as rapidly as those in Dissociative Identity Disorder.[2]:296
Schizophrenia includes a range of different possible symptoms and is a Psychotic Disorder, and a spectrum of Schizophrenia symptom disorders exist. All the Schizophrenia symptom disorders involve a break with reality. [2] In Dissociative Identity Disorder reality testing is described as being "in tact". Hearing voices, which are actually the communication of alter personalities is very common in DID, hearing voices may also present in Schizophrenia but in a slightly different way, and many of the symptoms historically used to diagnose symptoms of Schizophrenia are more common in Dissociative Identity Disorder - these are known as Schneiderian first-rank symptoms (FRS). See passive influence in Dissociative Identity Disorder for a description of these symptoms. Amnesia is a required symptom of DID but not a diagnostic symptom in Schizophrenia.[2]
Borderline Personality Disorder has many symptoms that overlap with the self-destructive behaviors common in Dissociative Identity Disorder, as well as symptoms that overlap with Complex PTSD (see below). The majority of people with Dissociative Identity Disorder also have Complex PTSD, and many have a diagnosis for Borderline Personality Disorder too (although these symptoms in DID may effect just the "host" identity or just specific alters).
Posttraumatic Stress Disorder is very common in people with Dissociative Identity Disorder, both should be diagnosed if both are present. Symptoms that may occur in both DID and PTSD are: amnesia for some aspects of trauma, flashbacks (i.e., a sense of disconnection from the present while reliving the trauma - for instance less awareness of the person's surroundings), and lastly the combination of post-traumatic symptoms of intrusion and avoidance, negative alterations in cognition and mood, and hyperarousal that are part of PTSD's diagnostic criteria. Symptoms of Dissociative Identity Disorder that are not found in PTSD are:
- 1) amnesias for many everyday (i.e., nontraumatic) events, which is greater than ordinary forgetfulness
- 2) flashbacks which are followed by amnesia for the traumatic content of the flashback
- 3) disruptive intrusions (unrelated to traumatic material) by alter identities into the individual's sense of self and agency, and
- 4) infrequent, full-blown changes (switches) between alters. [3]:296
- self-injury/self-mutilation, in DID this is more common in women/girls than in men/boys
- frequent suicidal behavior/suicidality, 70% of people with DID have attempted suicide
- dissociative flashbacks
- alterations in attention and consciousness (e.g. dissociation) - a core symptom in both conditions
- child abuse is a known cause of both Complex PTSD and DID, but not the only possible cause
- many comorbid disorders, especially depression, anxiety and substance abuse (drug abuse)
- borderline personality disorder co-occurs in around 33% of people with Complex PTSD and 30-70% of people with DID
- risk-taking or high-risk behavior
- interpersonal relationship problems may be a Functional Consequence of DID
- feelings of shame, which may involve underreporting symptoms (especially in DID)
- revictimization: experiencing violent or abusive relationships, including in adulthood
- somatization - physical illness or problems which are medically unexplained - a core symptom in Complex PTSD
Unexplained neurological symptoms are particularly common in DID, including non-epileptic seizures, Conversion Disorders (e.g., paralysis or sensory loss), and Somatic Symptom Disorders. The Somatoform Dissociation Questionnaire screening tool can help a clinician diagnose whether DID or OSDD is present. - body image distortions
In DID this may be linked to different identities: "Individuals may report that their bodies feel different (e.g., like a small child, like the opposite gender, huge and muscular). Alterations in sense of self and loss of personal agency may be accompanied by a feeling that these attitudes, emotions, and behaviors—even one's body—are 'not mine' and/or are 'not under my control'." [2]:293 - the core PTSD symptoms (required in Complex PTSD):
avoiding trauma reminders, re-experiencing trauma, negative thoughts/mood linked to trauma, problems with hyperarousal (e.g., being irritable or jumpy, sleep problems); most people with DID develop PTSD. [2]:280, 294-295, 297-298, [4], [5]:24, 127, 135-136, [7]:4, 11
Dissociative Disorders
See also: Full list of differential diagnoses for Dissociative Identity Disorder from the DSM-5 psychiatric manual.
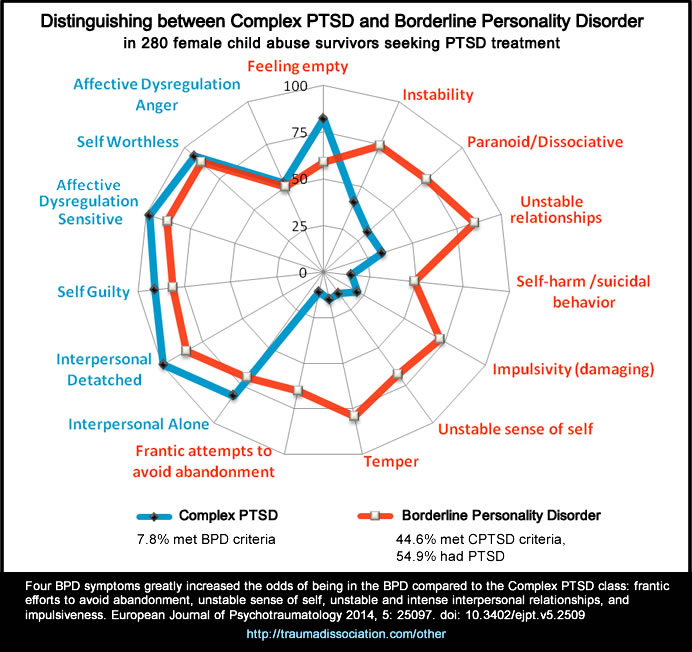
Borderline Personality Disorder
Borderline Personality Disorder (BPD) is a common misdiagnosis for Post-traumatic Stress Disorder and Dissociative Identity Disorder (DID).[2] While many people with BPD also have PTSD,[4] BPD may be diagnosed instead of, rather than in addition, to PTSD. Recent research has been shown clear differences between both PTSD and Complex PTSD and BPD. [3], [4] A key difference from Dissociative Identity Disorder is the presence of recurrent episodes of amnesia.[1], [2]
Comorbid Diagnoses
The majority of people with a Trauma or Dissociative Disorder also have other diagnoses at the same time, known as comorbid diagnosis.[2], [7]:606 Dual diagnosis is a term commonly used when a substance abuse disorder also exists, for example alcoholism. Conversion Disorder is common in people with Dissociative Disorders.
Posttraumatic Stress Disorder
Around 80% of people with PTSD have another psychiatric disorder at the same time. Depression, bipolar, anxiety or substance use disorders are common. [2]:280 Both substance use and conduct disorders are more common in males than females. U.S. military and combat veterans have high rates of Traumatic Brain Injury (TBI, caused by a physical head injury) occurring along with PTSD. [7]:606 In children, Oppositional Defiant Disorder and Separation Anxiety Disorder are the most common comorbid diagnoses.
Acute Stress Disorder
Extremely negative thoughts relating to the trauma are common, including excessive guilt for not preventing the trauma or not adapting successfully after trauma. Catastrophic thinking may occur, for example viewing flashbacks as a sign of reduced mental ability. Panic attacks, chaotic or impulsive behavior are common, for example reckless driving or making irrational decisions. Children may show separation anxiety. People who also have a mild Traumatic Brain Injury(mTBI) commonly experience post-concussive symptoms, such as headaches, dizziness, sensitivity to light/sound, concentration problems and irritability, all of which are also common in Acute Stress Disorder. [2]
Adjustment Disorders
These can occur along with almost any other mental disorder, provided the other disorder(s) do not fully explain the person's symptoms. Adjustment Disorders are commonly found in people with accompanying physical illness(es). [2]
Dissociative Identity Disorder
Most people with DID develop PTSD at some point, Complex PTSD symptoms are also very common.(despite not being classed as a separate disorder in the DSM). [2] , [5]:135 Depression, anxiety, and substance use disorders are commonly diagnosed in people with DID. Self-injury, non-epileptic seizures, conversion disorders and suicidal behavior are also common. [2]:7 294
Dissociative Amnesia
Many people with dissociative amnesia have PTSD at some point in their life, especially when the traumatic events prior to the amnesia are recalled. Somatic symptom disorders and conversion disorder are also common. Many people with this disorder have a personality disorder, with the most common being dependent personality disorder, avoidant personality disorder and borderline personality disorder.[2] When amnesia reduces more symptoms often become apparent, which may lead to other diagnoses such as persistent depression (dysthymia) or another depressive disorder, or Adjustment Disorder. Common symptoms include dysphoria, grief, rage, shame, guilt, psychological conflict/turmoil, suicidal or homicidal ideas and impulses. [2]
Depersonalization/Derealization Disorder
Depression and anxiety disorders are common. Rates of PTSD are low. The most common co-occurring personality disorders are avoidant, borderline, and obsessive-compulsive personality disorder. [2]
Somatic Symptom and related Disorders
Somatic Symptom and related Disorders, previously known as somatoform disorders, include prominent somatic (bodily) symptoms which cause significant distress or impaired functioning. These are physical symptoms and commonly treated with physical, rather than psychiatric, care. Many symptoms are medically unexplained, meaning they do not have a known medical cause at this point, however the physical symptoms are real and there are high rates of co-occurring physical health conditions in people with Somatic symptom disorder in particular. [2] Early traumas, including abuse, and genetics/biological vulnerability are known to contribute to these illnesses. This group of disorders are varied, and include Illness Anxiety Disorder (health anxiety which is severe enough to cause physical symptoms) and controversially also includes Factitious Disorder.
Somatoform Dissociation Questionnaire (SDQ)
The Dissociative Identity Disorder treatment guidelines suggest the SDQ, developed by trauma expert Ellert R.S. Nijenhuis, is helpful in aiding diagnosis of DID and Dissociative Disorder Not Otherwise Specified. [5]
Factitious Disorder DSM-5 code 300.19 (ICD-10 code F68.10) is a differential diagnosis for some disorders; this is intentionally and consciously falsifying either physical or psychological symptoms. It involves deception, and may involve intentionally inducing illness or injury or manipulating laboratory tests to indicate an abnormality where none exists. It is estimated to affect around 1% of people who are currently hospitalized, making it rarer than Dissociative Identity Disorder (for example), which affects 1-3% of the general population. [2], [5] Malingering is similar to Factitious Disorder but where external gain can be identified, for example time off work; malingering is not a mental illness. No estimates of prevalence are available in the DSM-5. Factitious Disorder and Malingering both involve deception. [2]
Conversion Disorder
This is also known as Functional Neurological Symptom Disorder, and involves "altered voluntary motor or sensory function" without a recognized neurological or medical cause but significant enough to cause impaired functioning or significant distress.. For example, loss of use of a limb. The ICD-10 psychiatric manual recognizes these as Dissociative [Conversion] Disorders, including weakness or paralysis, abnormal movement, speech or swallowing symptoms, sensory loss (including inability to feel pain). A psychological stressor may or may not be a known cause. Conversion Disorder includes psychogenic or non-epileptic seizures. Depersonalization, derealization, and dissociative amnesia are common. [2]
References
- World Health Organization. (1992). The ICD-10 Classification of Mental and Behavioural Disorders Clinical descriptions and diagnostic guidelines. Retrieved December 9, 2014, from http://www.who.int/classifications/icd/en/bluebook.pdf
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. (5th ed.). Washington, D.C.: American Psychiatric Association. ISBN 0890425558.
- Cloitre, M., Garvert, D. W., Brewin, C. R., Bryant, R. A., & Maercker, A. (2013). Evidence for proposed ICD-11 PTSD and complex PTSD: a latent profile analysis. European Journal of Psychotraumatology, 4(0). doi:10.3402/ejpt.v4i0.20706
- Cloitre, M., Garvert, D. W., Weiss, B., Carlson, E. B., & Bryant, R. A. (2014). Distinguishing PTSD, Complex PTSD, and Borderline Personality Disorder: A latent class analysis. European Journal of Psychotraumatology, 5(0). doi:10.3402/ejpt.v5.25097
- International Society for the Study of Trauma and Dissociation. (2011). Guidelines For Treating Dissociative Identity Disorder In Adults, Third Revision: Summary Version. Journal of Trauma & Dissociation,12(2), 188-212. DOI: 10.1080/15299732.2011.537248.
- Foa, E., Keane, T., Friedman, M., & Cohen, J. (Eds.). (2009). Effective treatments for PTSD: Practice guidelines from the International Society for Traumatic Stress Studies (2nd ed.). New York: Guilford Press. ISBN 9781606237922.
- Cloitre, M., Courtois, C.A., Ford, J.D., Green, B.L., Alexander, P., Briere, J., Herman, J.L., Lanius, R., Stolbach, B.C., Spinazzola, J., Van der Kolk, B.A., Van der Hart, O. (2012). The ISTSS Expert Consensus Treatment Guidelines for Complex PTSD in Adults. Retrieved from December 10, 2014 http://www.istss.org/ISTSS_Main/media/Documents/ComplexPTSD.pdf
Cite this page
Other Disorders. Traumadissociation.com. Retrieved from .This information can be copied or modified for any purpose, including commercially, provided a link back is included. License: CC BY-SA 4.0
